Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease that affects nerve cells in the brain and the spinal cord. Furthermore, it results in the degeneration of upper and lower motor neurons responsible for voluntary movements and muscle control, resulting in progressive loss of speech, atrophy, fasciculations, and eventually respiratory failure when diaphragm and chest muscles fail. While about 10 percent of those with ALS survive for 10 or more years, most people with ALS die from respiratory failure, usually within 3 to 5 years from the onset of symptoms. There are two different types of ALS, sporadic and familial. Sporadic which is the most common form of the disease in the U.S., is 90 – 95 percent of all cases. It may affect anyone, anywhere. Familial ALS (FALS) accounts for 5 to 10 percent of all cases in the U.S. At present, there is no cure for ALS and most treatments are designed to relieve symptoms and improve the quality of life for individuals with the disorder. That being said, how far should treatment go given the invariably fatal nature of this disorder and the associated degree of paralysis?
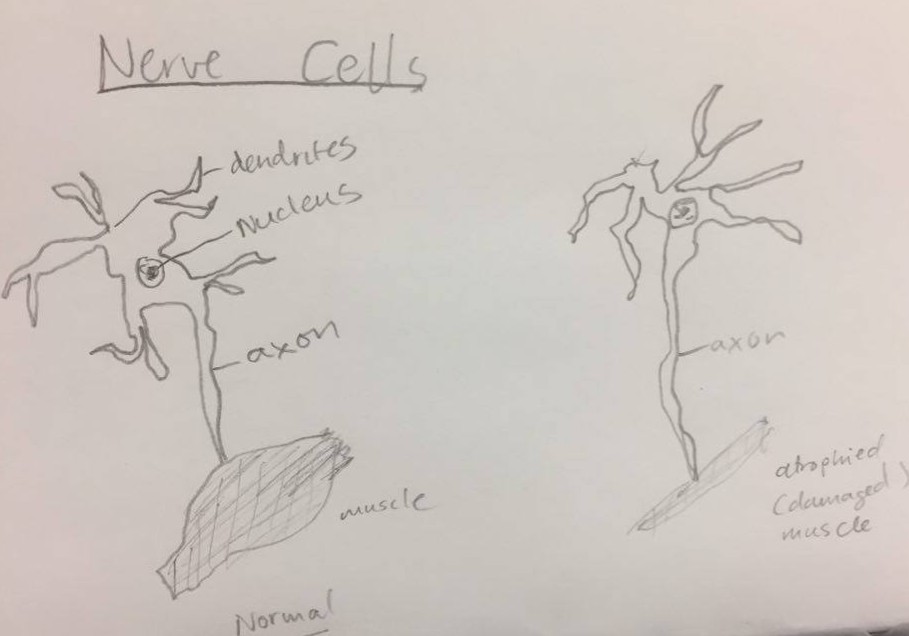
Given a choice, most people would prefer to prolong their lives for as long as humanly possible, largely in the hope of a medical miracle bringing them back from the brink of death, possibly to their former self or a similar rendition of the same. In the case of ALS, death is slow but certain, and in its late stages, patients experience total paralysis, including that of chest wall and diaphragm muscles (See diagram below of atrophied muscle in ALS). At this point, one may argue that there is still some sentimental value to the physical presence of one’s loved one regardless of their physical state. In my view, furthering the life of a late stage ALS patient on a long term basis is an impractical and unsustainable route for all parties involved. In the case of few patients that can afford the medical care, only the health care institutions benefit from the situation while friends and family incur extremely steep financial costs. In the larger share of patients who cannot afford being placed on a ventilator and being continually hospitalized, their bill becomes the responsibility of the state and health care infrastructure as a whole, an all round lose-lose scenario for all parties involved.
In precis, while my position may sound insensitive to some, or shallow on the account that I write from a third party viewpoint, it is imperative for this discussion to be initiated and sustained. Also, families in this predicament ought to be earnestly well informed about the contours of the journey they are on through conversing with social workers and the health care professionals serving their loved ones. While civilization has made huge leaps and bounds to prolong life through the ingenuity of medical researchers in disciplines such as surgical, pharmaceutical, and nutrition research, it is also incumbent upon ourselves to perform cost benefit analyses such that we avoid engaging in futile cycles in which we continue to expend financial and other resources to sustain life at all costs, even though the nature and quality of life may deteriorate to less than a shadow of its former glory.
Below is a diagram of muscular differences between normal and ALS diseased muscle.
Life Is Priceless, Sure, How Far Should We Go to Prolong It Though?

Chilling to hear that life and appropriate medical care comes down to a “cost-benefit” analysis. If you take the logic of your argument and expanded to other situations then what happens to the elderly with dementia, for example?
Good point, Mark. I won’t answer your question for the student but wanted to share my thoughts on our discussion last week. It was a tough one 🙁
A natural death is the desire of many. However, with the advances in medicine, we discussed how with our ability to prolong life and treat disease, it feels like we have caused a shift in when -and even how- that natural endpoint occurs. Perhaps as a result, many families now find their loved ones battling diseases that are associated with aging. Like dememtia.
We talked about ALS this week; it was sad and depressing honestly. It did bring up cost-benefit, which is uncomfortable for me, and I would agree with your describing it as chilling. As I reflect on it more deeply, I only know that when love is felt -and shared- between patient and those dear to them…that is living.
Thanks for the discussion, Mark 🙂
Mark, first of all I appreciate your response and can certainly relate to your assertion. I guess my worries about coming off as a tad bit cold were not out of wack, good to know 😀 I do want to question the term you used “appropriate” medical care. What is truly appropriate? Is it a ventilator on a fully paralyzed and unresponsive ALS patient for 3 years? Life is invaluable, we all agree, I do think that medical advances have allowed us to play God, to defy the biological forces of survival of the fittest and to basically play hide and seek with the circle of life.. When I speak of a cost-benefit analysis, I am considering beyond the dollar amount, to say how far are we willing to go to delay the inevitable? Human relationships have a social element to them, which really is the flame that keep them going. If all I have left with a relative with ALS is just physically seeing them with no dialogue in any shape of form, with their existence permanently and artificially mechanized, and the slope of it all invariably downward, I do worry about what is the “appropriate” extent to reach. As much as we are natural procrastinators, I do really feel like the law of diminishing returns applies to our artificial and unsustainable methods of prolonging life.