Medical Marijuana vs. Recreational Marijuana
Use of the hemp plant has been dated back to 6000 B.C. for its consumption of seeds and use for textiles. The first recorded use of cannabis as medicine was in 2727 B.C. in China for a variety of health problems.
Marijuana/hemp plant originated in 600 B.C. in Asia for its common use in religious ceremonies or healing practices by most people. It was later brought to North America in the 1500s by the Spanish. In 1937, the Marijuana Tax Act was implemented that decreased the accessibility and affordability of marijuana. President Nixon repealed this act who later made it a Schedule I drug in 1970.
Medical Marijuana is the whole unprocessed weed plant of more than 100 different cannabinoids. Even though it is medical, it is not FDA approved. Medical marijuana has higher levels of CBD than THC. You must have a prescription from a doctor, be over 18 and marijuana must be legal in the state for medical use. [Legal in thirty-two states]
Recreational Marijuana is the usage of pot without any medical justification. Recreational marijuana tends to have higher levels of THC than CBD for the “high.” You must be 21 years old and marijuana must be legal in the state for recreational use. [Legal in ten states]
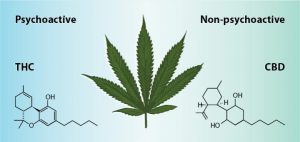
CBD vs. THC
CBD (cannabidiol): is a naturally cannabinoid found in hemp plants. Has no psychoactive effects and has very little to no side effects due to its extremely high tolerance for CBD is legal in all 50 states when extracted from a hemp plant that contains less than 1% of THC.
THC (tetrahydrocannabinol): is a the main psychoactive component of marijuana. It binds with CB1 causing a euphoria effect.
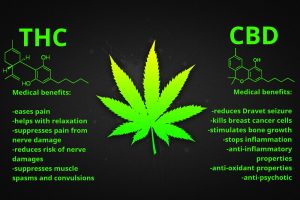
Benefits & Pathways
Obesity: When the CB1 receptor is stimulated the desire to eat is increased. CBD is an antagonist for the CB1 receptor but also has a low affinity for the receptor. When cannabidiol binds to the CB1 receptor it suppresses the feeling to intake food. For marijuana to be a treatment for obesity it must have a higher concentration of CBD than THC to decrease the desire to eat.
Migraine: THC, an agonist for the CB1 receptor, can bind to CB1 reducing the first few symptoms preceding migraines. However, it is unknown how the psychoactive properties of THC play a role in treatment of cluster headaches.
Pain Reduction: THC will activate CB1 that decreases the TRPV1 (vanilloid receptor) channel. CBD will inhibit CB1 that then inhibits FAAH that leads to desensitizing TRPV1 channel. There is a decrease of calcium influx resulting in less pain.
Anti-Cancer: CB1 and CB2 receptor agonists increase this apoptotic cell death in glioma cells. ER stress may also be activated intrinsic apoptosis pathway.
Anti-Anxiety: CBD increases signaling through 5-HT1A (serotonin receptors). A reduction in anxiety and a mood boost is seen. Due to its increase of serotonin signaling it can also be seen as a treatment for depression.
Research: A continuation and increase of research on marijuana is needed for a more conclusive statement. Unfortunately, with it being a schedule I drug it is difficult to access the drug as well as get approval for the research. Hopefully, in the future there will be in an increase of knowledge and regulation of marijuana. With increased research, there is a hope for the use of marijuana for its various benefits.
References:
- What is the Difference Between Medical and Recreational Marijuana? DocMJ. 2017. https://docmj.com/2017/06/05/difference-medical-recreational-marijuana/
- CBD vs. THC: What is the Difference? HealthLine Red. https://www.healthline.com/health/cbd-vs-thc#at-a-glance
- Fonseca, BM, et al. “Endogenous cannabinoids revisited: A biochemistry perspective.” Prostaglandins and Other Lipid Mediators, vol. 102-103, 2013, http://dx.doi.org/10.1016/j.prostaglandins.2013.02.002