Marijuana has long been used recreationally and medicinally. While its recreational use is still of debate, its medicinal properties have also come under great study, especially in recent years. The active components in marijuana act on the bodies endocannabinoid system, comprised of the receptors cannabinoid receptor 1 and 2 (CBR1 and CBR2). There are around 70 phytocannabinoids that have been identified in the marijuana plant, but ∆9-tetrahydrocannabinol (THC) is the main psychoactive component. THC has long been the barrier to effective medicinal use of marijuana, although deeper research suggests there are additional hurdles.
Endocannabinoids
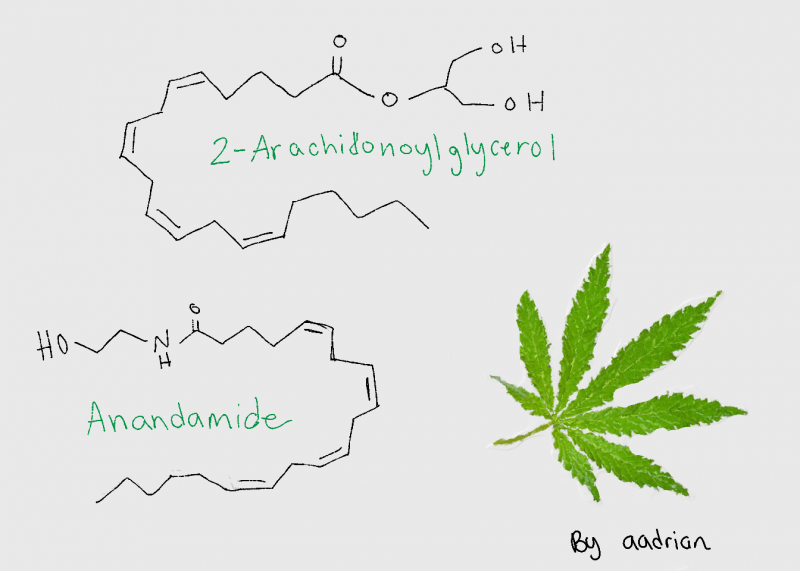
Endocannabinoids, or the endogenous agonists of the CBRs, in the human body are anandamide (AEA) and 2-arachnidonoylglycerol (2-AG). These are the chemicals that are synthesized inside the brain and act on the CBRs in response to various signaling events. CBR1 is the dominant receptor in the brain and muscle, with other isoforms in tissue like the liver and pancreas. CBR2 is present in brain reward regions, the testis, and spleen, depending on the isoform. Because there are multiple forms of both receptors and they are expressed at significant levels in many different tissues, it becomes more difficult to target a specific response from the endocannabinoid system. Depending on the endocannabinoid, they also act and target the receptors differently. AEA has been shown to be a high-affinity partial agonist of CBR1, meaning it binds at low concentrations but only has a partial effect; it is also almost entirely inactive at the CBR2. 2-AG, however, acts as a full agonist of both receptors but at moderately low affinity. Both endocannabinoids are produced on demand in response to increased intracellular Ca+2 concentrations, which means this system can be activated from a variety of upstream effects. The full paper that reviews these topics and more can be found here.
Medicinal Use of Endocannabinoids
The effects of the endocannabinoid system based on single cell activation is extremely varied, as is demonstrated in this graphic.
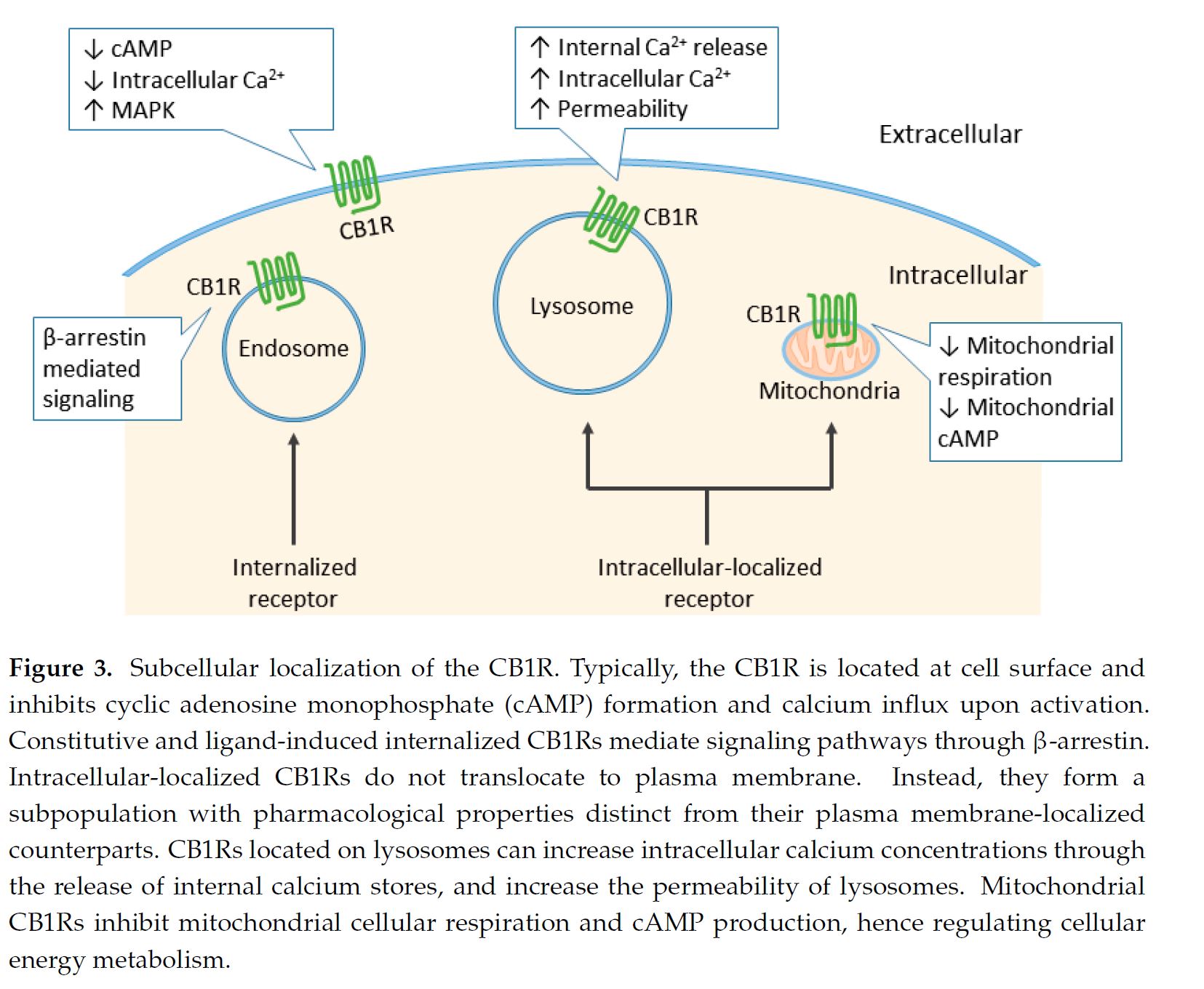
Not only can these receptors be activated by a ligand binding on the extracellular side, but there has also been activity shown on internally localized receptors, whether those were taken in through endosome processes or if they were intrinsically localized on a lysosome or mitochondria. This is another reason why targeting the CBRs for medical use is difficult.
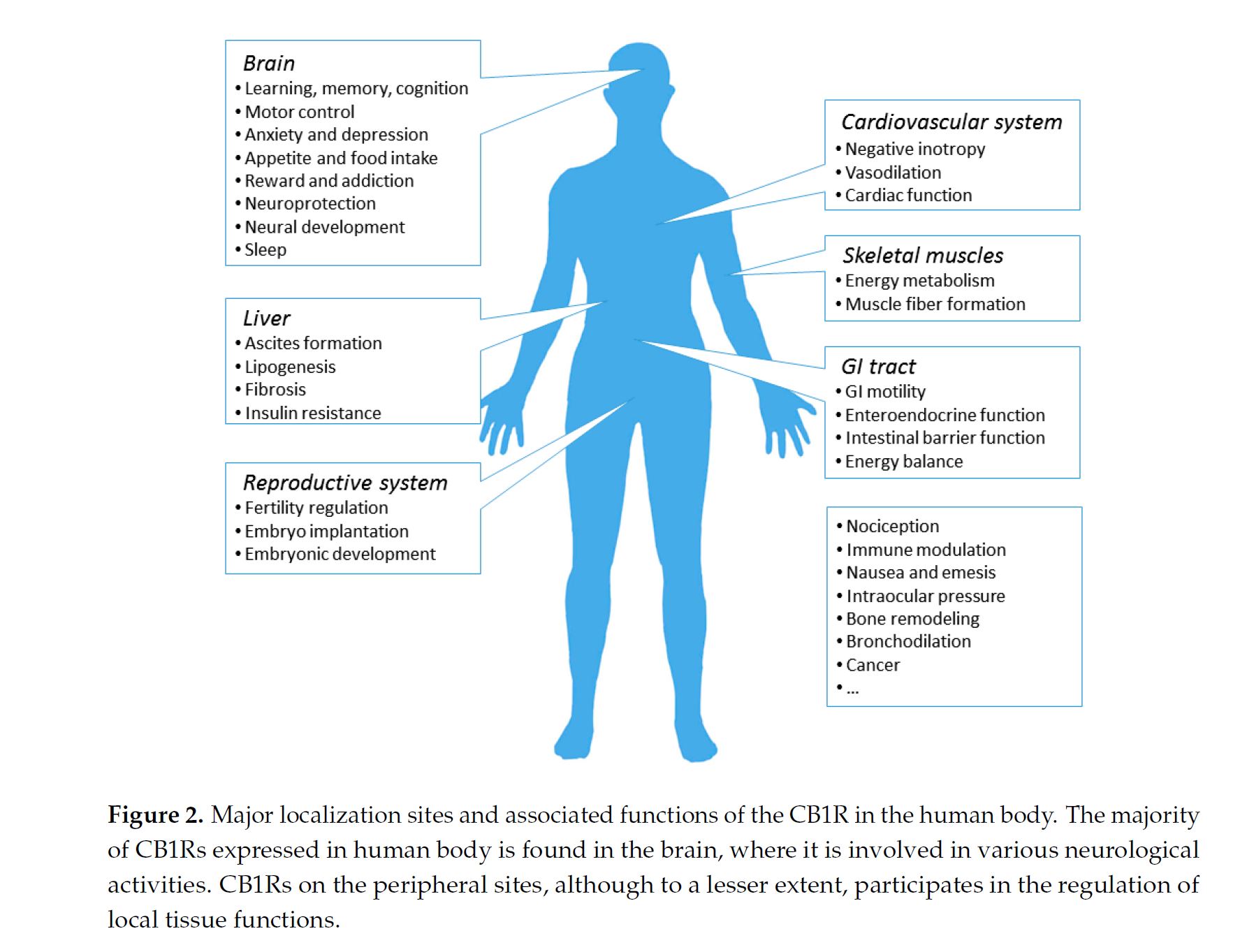
Cell signaling pathways through β-arrestin and other methods result in different cellular effects that might be off of the intended process. In addition to their highly distinct roles and locations in the cell, they are also found around the body with different affects, depending on the location and cell type.
What does it mean?
In the end, while medical marijuana is currently being marketed as a miracle for conditions from multiple sclerosis, to seizures, to palliative cancer care, the science is less clear. Our understanding of the signaling processes, especially the non-GPCR alternate pathways, is limited. Until we are able to elucidate the pathways more succinctly and understand the downstream effects, positive development of cannabinoid pharmaceuticals will be limited.