Artstract Created by Hailey Puppe
Glioblastoma is an aggressive, fast-growing malignant brain tumor. It has a very low survival rate. Only 5% of those with Glioblastoma will live past 5 years. Treatment usually consists of surgery, radiation, and chemotherapy.1
There are two main types of Glioblastoma, primary and secondary.
- Primary Glioblastoma effects elderly people and represents around 90% of Glioblastoma cases. This is characterized by EGFR amplification and is fast growing and very aggressive. EGFR is epidermal growth factor receptor. Overexpression allows for continual cell growth.
- Secondary Glioblastoma effects younger people. First signs of this appears in childhood prior to puberty. Children will often experience excessive headaches. Once children reach puberty, the tumors will die out. Unfortunately, these tumors come back later, prior to 50 years of age. Secondary Glioblastoma has a better response to chemo than primary due to a genetic component that shuts off DNA repair that occurs after damage done by chemo treatment. This allows the tumors to die.
Pathways Involved
In Glioblastoma there are a few things that go wrong in signaling. As discussed previously, EGFR is amplified in Glioblastoma. This leads excess cellular signaling to produce new cells. Some pathways included in this are cAMP, MAPK, and PI3K.
- When a ligand like epidermal growth factor bind to the RTK receptor, signaling occurs that activates RAS. In turn, RAS activates RAF, MEF, and then MAPK. MAPK then activates CREB to lead to cell production. In Glioblastoma, MAPK becomes hyperactivated which leads to increased cell production.
- When a growth factor binds to the RTK receptor. PI3K is recruited to the receptor and allows for cellular signaling in the cell that leads to CREB becoming activated. In Glioblastoma PI3K amplified and CREB is hyperactivation causes increased cell production.
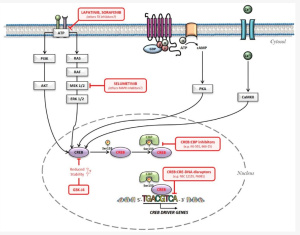
- When a ligand binds to the G-coupled protein receptor, adenylyl cyclase converts ATP to cAMP. cAMP activates PKA which inhibits tumor growth by activating gene transcription. cAMP is lower in Glioblastoma and cannot activate PKA. PDE degrades cAMP in Glioblastoma and tumor growth is not inhibited.1
Each of these pathways can be targeted for the treatment of Glioblastoma. This figure shows how each pathway is involved in gene transcription and how different medications may effect these pathways.
Possible Treatments
Two major factors involved in increased cell production in Glioblastoma is EGFR amplification and CREB hyperactivation.
EGFR gene amplification is also found in other cancers. Unfortunately, targeting EGFR in cancer treatment has not shown to be effective against Glioblastoma. EGFR inhibitors have helped with other cancers, but trials with Glioblastoma have not shown promise. A specific genetic variant of EGFR, ΔEGFR, is specific to tumors. Treatment with a ΔEGFR monoclonal antibody has shown to decrease tumor growth and increase cell death.2
CREB inhibition on the other hand shows more promise. Other medications that inhibit signaling in RTK receptors leads to decreased CREB activation. This was shown to decrease tumor cells. CREB inhibitors are currently in pre-clinical trials for the treatment of cancer and could be a potential treatment of Glioblastoma.3
Glioblastoma is a very aggressive and difficult disease to treat. Exploring the different pathways involved in Glioblastoma can provide new solutions to treatment. Targeting EGFR and CREB has shown some promise, but different aspects of these pathways need additional discovery.