Glioblastoma (GBM), a cancer of the astrocytes which support brain neurons, is the most common brain cancer. This cancer is particularly difficult to treat due to its highly invasive nature, the cellular heterogenicity of the tumors and the vital signaling pathways that the cancer manipulates. For these reasons GBM can be very difficult to treat, leading it to be a cancer with one of the worst survival rates. Novel treatment options are being developed with hopes to improve survival rates by manipulating signaling pathways that are aiding in the development of these cancer cells such as the MAPK, PI3K, and cAMP pathways [3].
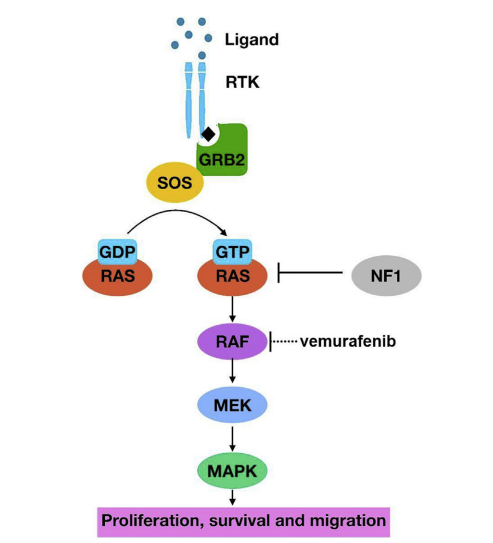
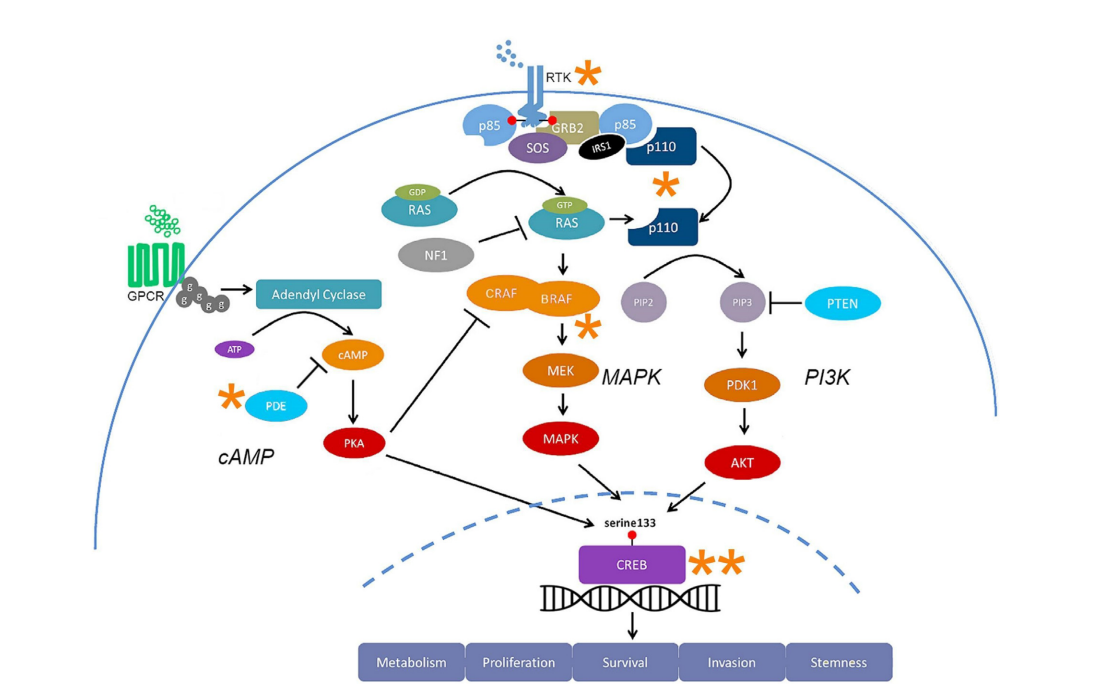
Figure 1: The MAPK pathway begins with a ligand binding to an RTK receptor, which allows for the SH2 domain of the adaptor protein to bind and recruit SOS. SOS exchanges GDP for GTP, activating RAS and the kinase cascade. Vemurafenib is a drug used to inhibit RAF in GBM treatment. [3]The MAPK pathway (Figure 10 is a receptor tyrosine kinase (RTK) pathway that regulates cell proliferation, cell survival, and metastasis. When this pathway is overactive, GBM prognosis is worsened. This pathway can be affected at different points in the process which can elicit different results. The epidermal growth factor (EGFR) gene is commonly upregulated in GBM. EGFR is a growth factor ligand that binds to the RTK receptor and activates the signaling process. Similarly, NF1 (a negative regulator of the pathway) is absent or inactive in some GBM cases which also will allow for greater MAPK signaling [3].
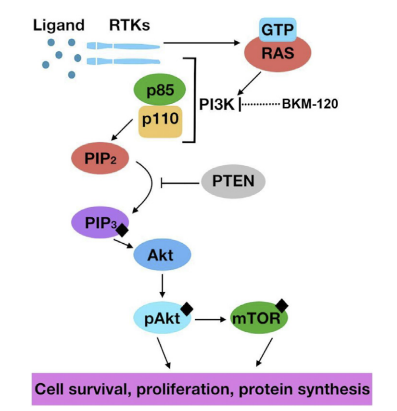
The PI3K pathway (Figure 2) is another RTK pathway that is overactive in GBM. When PI3K activation occurs, it leads to activation of Akt and mTOR, synthesizing proteins which can stimulate cancer cell growth. For this reason, BKM120 is a drug that is used to inhibit PI3K [3].
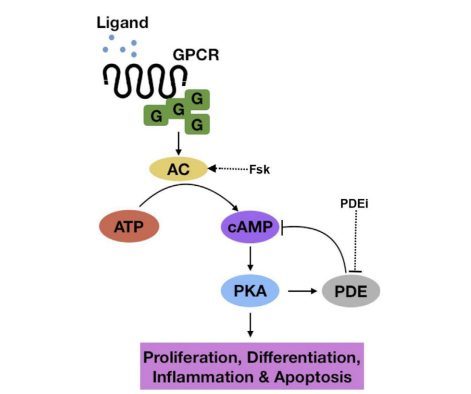
Figure 2: PI3K activation begins with a ligand binding to an RTK receptor which recruits GTP-activated RAS to begin the signaling process which can result in cellular growth and proliferation. [3]Figure 3: The cAMP pathway is a GPCR pathway that can aid in cellular regulation of apoptosis, inflammation, differentiation, and proliferation. [3]A third pathway related to GBM development and treatment is the cAMP pathway. Unlike the previous pathways, cAMP tends to e under-activated in tumors. This pathway uses a G-protein coupled receptor (GPCR) which, when activated, uses adenylyl cyclase to convert ATP into cAMP, a second messenger. This pathway is negatively regulated by phosphodiesterases (PDE). In order to increase the amount of cAMP, which can induce apoptosis of cancer cells, PDE-inhibitor drugs are used [3].
The MAPK, PI3K, and cAMP pathways all converge at CREB (Figure 4), a transcription factor that is positively correlated with patient survival of malignancies. Therapeutic interventions targeting this convergence could be very effective at treating these signaling dysregulations associated with GBM. Utilizing nodes of convergence between pathways as treatment targets may also reduce the toxic load associated with chemotherapies [3].
Figure 4: The MAPK, PI3K and cAMP pathways all converge at the transcription factor CREB. Upregulation of CREB is a potential treatment target that can mitigate the proliferation of cancer cells. [3]Because of the heterogenous nature and adaptability of cancer cells and GBM cells specifically, utilizing a single drug with a single target that could affect multiple pathways could be extremely helpful in improving the survival rates with these types of cancers.
(3) Fung, N. H.; Grima, C. A.; Widodo, S. S.; Kaye, A. H.; Whitehead, C. A.; Stylli, S. S.; Mantamadiotis, T. Understanding and Exploiting Cell Signalling Convergence Nodes and Pathway Cross-Talk in Malignant Brain Cancer. Cellular Signalling2019, 57, 2–9. https://doi.org/10.1016/j.cellsig.2019.01.011.
(6) Fruman, D. A.; Chiu, H.; Hopkins, B. D.; Bagrodia, S.; Cantley, L. C.; Abraham, R. T. The PI3K Pathway in Human Disease. Cell2017, 170 (4), 605–635. https://doi.org/10.1016/j.cell.2017.07.029.