OH NO!- Comorbidity!
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition that is known for its challenges in social situations such as social communication, repetitive behaviors, and problems with social cues. Those with ASD have difficulty expressing and understanding emotions, however this expands beyond the normal symptomology
Comorbidity is an additional disease on top of a primary diagnosis. They are more common in those with ASD than those without. Research shows a high rate of comorbidities- about 70% of those with ASD have co-occuring conditions that blur diagnosis and treatment for patients with ASD. Symptoms that develop with comorbidities add to the original symptoms of ASD making a healthy life difficult to have.
Genetic complexity
Autism does not have a single genetic cause. The developmental disorder is influenced by a multitude of factors. Primarily, multiple genetic factors like genetic mutations or copy number variations (CNVs). CNVs are a type of structural variation in the genome where DNA is deleted or duplicated. This changes normal function of genes and changes the number of gene copies present therefore, leading to developmental issues.
Fragile X Chromosome (FXS)
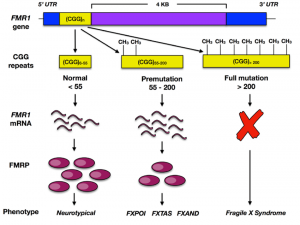
FXS is one condition that is associated with autism that is linked with DA dysfunction. It is the number 1 inherited cause of a wide range of intellectual disabilities. 1 in 3 individuals with ASD have FXS. This condition results from the repetition and mutation of the gene FMR1 which null mutants have significant increase in the synthesis of DA and 5-HT which is another name for serotonin- a neurotransmitter in charge of various functions including mood and helping out the nervous system.
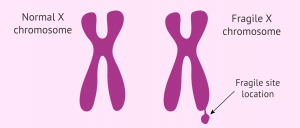
In Figure 2, a typical chromosome the FMR1 gene will repeat just enough to maintain regulation for CGG repeat sequence, which will not interfere with functioning of the gene, however, a fragile X chromosome will exceed the number of regulated CGG repeat sequence and the FMR1 gene will slice, leaving an absence of the gene. Without the FMR1 gene neurons struggle to make synaptic connections in the brain.
When working with CNV’s you’re working with a lot of DNA! CNV’s make large changes to genetic material. This is one of the reasons why they are common in people who are neurodivergent. These genetic risk factors result in subtypes that ultimately have a cascade of behavioral symptoms. For example, deletion of specific gene like 16p11.2 can result in delayed speech and struggling with social intelligence. So rather than focus on one gene, like finding a needle in a haystack, its better to try and adapt and understand the subtypes and comorbities of ASD.
The Role of Dopamine and Dopamine Transporter DAT
Dopamine (DA) is a widely known neurotransmitter that influences an array of functions within the brain. As one of the top three numerous neurotransmitters found in the brain, dysfunction of this molecule can lead to neurodevelopemental and psychiatric disorders including Autism. Too much or too little dopamine in those with ASD cause symptoms such as issues with sensory processing, repetitive behaviors, motor control and social reward processing.
There are two primary dopamine receptors, D1 and D2. These receptors are critical for managing the effects that dopamine has on the brain. Dysfunction of these receptors has been proven to be linked in ASD. These two receptors contribute mainly to behavioral disruptions that are present in ASD such as, social deficits, behavioral flexibility, and cognitive attention.
D1 vs D2
D1 Receptors: During activation D1 receptors are primarily known for their synaptic plasticity, the strength in connection between neurons, and facilitating excitatory signaling, which is increasing neural activity. Synaptic plasticity and facilitating excitatory signaling regulates executive function and cognitive flexibility. They’re crucial for learning and memory. Dysfunction in D1 leads to deficits in communication and attention.
D2 Receptors: Unlike D1 receptors, D2 is mainly involved inhibitory signaling-which is the decrease of neural activity- and involvement with motor control and coordination, in ASD, an overactive reward system leads to repetitive behaviors. In this situation the brains reward pathways are eing hyperstimulated and overly sensitive. When D2 receptors are not functioning there is no ‘manager’ to modulate motor control and coordination within movements.
DAT is the dopamine transporter in charge of regulating dopamine. The process in which dopamine levels are regulated from the synapse back into the neuron This means a dysfunction in DAT is a dysfunction in dopamine signaling. DA signaling drives behavioral activation which increases with reward rate.
What does This Have to do With Comorbidities?
ASD and its comorbid conditions can help research within dopamine receptors to understand where dysregulation occurs. ASD contributes to neurological development of existing disorders as behavior, cognition, and emotion are all affected. Comorbidities are harmful to an individuals quality of life as with autism, it can be difficult to express how you are feeling. If we evaluate dopaminergic dysfunction we can understand core symptomology and be closer to the answer.

Al-Beltagi M. (2021). Autism medical comorbidities. World journal of clinical pediatrics, 10(3), 15–28. https://doi.org/10.5409/wjcp.v10.i3.15
DiCarlo, G. E., & Wallace, M. T. (2022, February). Modeling dopamine dysfunction in autism spectrum disorder: From invertebrates to vertebrates. Neuroscience and biobehavioral reviews. https://pmc.ncbi.nlm.nih.gov/articles/PMC8792250/
Hunter, J. E. (2024, May 16). FMR1 disorders. GeneReviews® [Internet]. https://www.ncbi.nlm.nih.gov/books/NBK1384/