CONCUSSIONS are one of the most commonly encountered sports injuries where rates are estimated at two million sport related concussions per year in the United States according to the Brain Injury Research Institute. This number is potentially much larger due to the lack of knowledge and awareness about concussion and brain injuries. There has been an increase in research attempting to understand what happens in the concussed brain, but there is a long way to go to help identify treatment plans and return to play protocols. For now, we maybe shouldn’t listen to Zac Efron and his High School Musical buddies. So let’s keep our head out of the game and, instead, focus on raising awareness about concussions and other injuries to the brain.
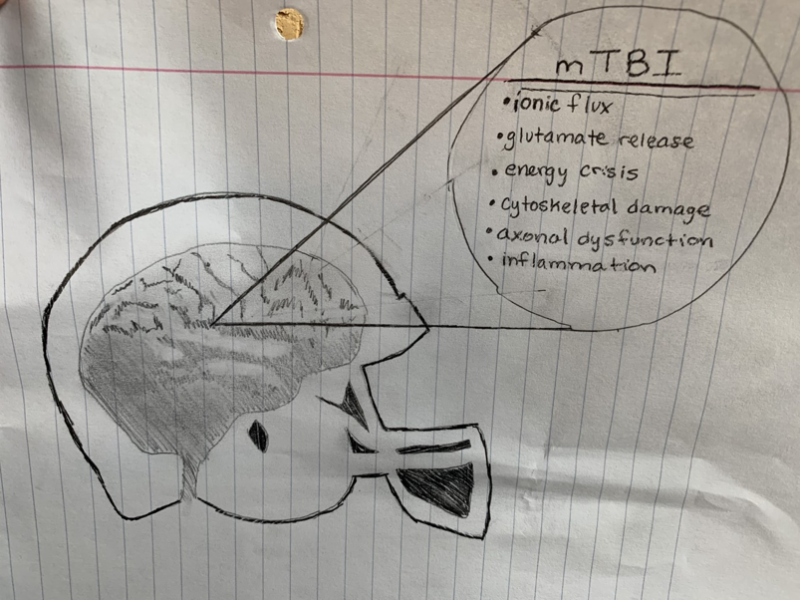
A vast array of symptoms that can be associated with concussions and traumatic brain injuries (TBI) are a result of the diversity and broadness of factors relating to basic neurobiology and a neurometabolic cascade. These factors include ionic flux and glutamate release, energy crisis, cytoskeletal damage, axonal dysfunction and altered neurotransmission, and inflammation.
IONIC FLUX AND GLUTAMATE RELEASE
Upon a biomechanical injury, potassium efflux and sodium and calcium influx occur due to a damaged phospholipid membrane. An efficient action potential will not be able to be produced because of abnormal depolarization from the rapid influx of sodium and calcium.
ENERGY CRISIS
In an effort to maintain cellular homeostasis regarding ionic flux, ionic pumps that require ATP are shifted into overdrive. This leads to a depletion of energy reserves, thus resulting in reduced cerebral blood flow and an imbalance between energy supply and demand. Prolonged calcium influx leads to increased intracellular calcium and greater amounts of calcium to be sequestered in the mitochondria. Too much sequestration can result in mitochondrial dysfunction which causes the energy crisis.
CYTOSKELETAL DAMAGE
The cytoskeletal structure which include microtubules and microfilaments consist of delicate and complex components. When damage is implemented to a brain region, neurofilaments can easily be phosphorylated and break. Axonal influx of calcium results in the breakdown of proteins into smaller polypeptides on cytoskeletal components. This damage makes the neurons more prone to axonal disconnection and death. After a TBI, ongoing cerebral and hippocampal atrophy may be present. The progressive atrophy can show the appearance of cognitive deficits later in life. The occurrence of a TBI before full recovery from a previous TBI may more likely trigger activation of intracellular proteases and the cascade that leads to apoptotic cell death.
AXONAL DYSFUNCTION AND ALTERED NEUROTRANSMISSION
Increased axonal permeability after a TBI is a result of the vulnerability of the axon. Consequently, this can lead to overall axonal dysfunction. A damaged neuron where neurofilaments and microtubules are altered allows for the neuron to not normally function. Injury to the axon and other white matter areas occurs along with mechanoporation, stretching of individual axons, disruption of axonal transport, axonal misshaping, and axonal disconnection.
Altered neuronal transmission is present after a TBI and occurs due to an imbalance in excitatory and inhibitory neurotransmission. This imbalance is seen due to alterations in the glutamate receptors or GABA receptors which alter excitation and inhibition. Alterations in glutamate, an excitatory neurotransmitter, affect the normal functions of calcium flux and the activation of downstream signal transduction molecules. Decreased levels of GABA, an inhibitory neurotransmitter, affect fear-based learning associated in the amygdala.
INFLAMMATION
Changes in inflammatory markers following a TBI has shown an activation of microglia in the cortex. Microglia function as macrophages in the central nervous system to mediate immune responses. Upon damage to the brain, inflammatory changes are triggered by the upregulation of cytokine and inflammatory genes. Inflammation, although an evolutionary mechanism for protection, has also been shown to induce damage to brain regions that relate to long term side effects. For example, microglial response to damage in the substantia nigra has been shown to increase risk of Parkinson’s Disease after a TBI.
WHY IS THIS SO IMPORTANT?
The research presented above sheds light onto why there are so many symptoms involved with brain injury and concussion. A list of symptoms is listed below:
- Migraine headache
- Photophobia and phonophobia
- Vulnerability to second injury
- Impaired cognition
- Slowed processing and slowed reaction time
- Chronic atrophy
- Development of persistent impairments
Concussions affect each individual differently and symptoms depend on a number of factors including strength of trauma and the brain area affected by the trauma. When an individual is experiencing these symptoms, they must be monitored closely. Both physical and mental rest can speed the recovery of concussions. Unfortunately, there is still much more research to better understand how to prevent concussions and the symptoms associated with them.
CONCUSSIONS and any injury to the brain are not to be taken lightly. The broadness of symptoms associated can have long term affects. Management of concussions will continue to evolve as more research develops. This will allow us to better understand the steps toward prevention, treatment, and return to play protocols. Protection of athletes and all those more prone to concussion is the number one priority. If you are experiencing any of the concussion symptoms talk to a health professional and play it safe by getting your head out of the game!
For more information on the research presented, follow:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4479139/
For more information on the symptoms associated with concussion, follow:
https://www.mayoclinic.org/diseases-conditions/concussion/symptoms-causes/syc-20355594