
Pre-knowledge before using naltrexone
Naltrexone is an opioid antagonist that is not addictive and does not cause withdrawal symptoms with the use of stopping it. Naltrexone blocks the euphoric and sedative effects of opioid receptors and reduces opioid craving. Before starting Naltrexone, an individual needs to wait 7 days after their last use of short-acting opioids and 10-14 days for long-acting opioids and alcohol. Accidental or intentional ingestion of naltrexone in opioid dependent people will result in an acute block of opioid receptors and precipitate a severe opioid withdrawal reaction. Symptoms of withdrawal can appear after only five minutes following ingestion and may last up to 48 hours.
How was naltrexone created?
Naloxone, the long-acting naltrexone is a MOR antagonist. It was first synthesized in 1963 by Endo Laboratories. Though the drug remained essentially dormant for several years, it attracted interest in 1972 when Congress passed the Drug Abuse Office and Treatment Act for the purpose of developing non-addictive treatments for heroin addiction. At that time, methadone, a long acting MOR agonist, was the only medication available for opioid addiction. It seemed to stop cravings yet not produce as significant of a “high” or cognitive inhibition of heroin. However, in some cases individuals did report having experienced some of these cravings.
How does naltrexone work?
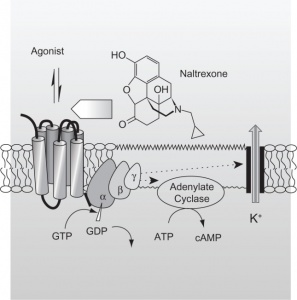
Repeated exposure to drugs of abuse can lead to an increase in delta FosB levels that persist for a long time after the cessation of drug treatment. To give a little background, research has found that the transcription factor of delta FosB is a mechanism that drugs of abuse produce changes within the brain the contribute to the addiction phenotype. FosB transcription factors accumulate within the nucleus accumbens and dorsal striatum. These brain regions are heavily impacted by repeated drug abuse. https://pubmed.ncbi.nlm.nih.gov/11572966/
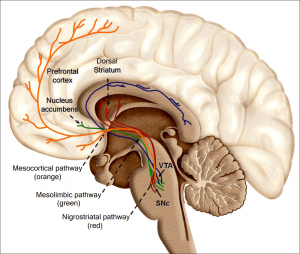
Naltrexone attenuates ethanol consumption via antagonizing the down regulation of CaM kinase IV and the phosphorylation of CREB in the striatum region induced by forced ethanol exposure. Naloxone increases the firing of VTA dopamine neurons by inhibiting VTA GABAergic interneurons. It has been shown that μ opioid receptor agonists indirectly increase dopamine release in NAc and caudate putamen and that the induction of delts FosB by psychostimulants is mediated by D1 dopamine receptor pathway. Furthermore, naltrexone attenuates striatum dopamine levels, which are increased by systemic administration of ethanol. Therefore, naltrexone-induced attenuation of dopamine levels may contribute to its attenuation of FosB/delta FosB IR upregulation observed in current study. In summary, the present study demonstrates that chronic voluntary consumption of large quantities of ethanol induces FosB/delta FosB expression selectively in the subregions of the striatum and the prefrontal cortex, which is reversed by naltrexone treatment. https://www.pnas.org/content/85/14/5274.short. https://www.sciencedirect.com/science/article/pii/S0014299904002249
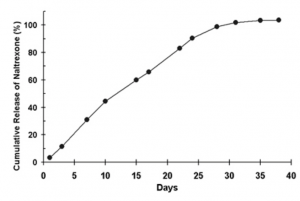
Figure 1. Representative in vitro drug release profile of the lead formulation of extended-release naltrexone.
A near linear in vitro release profile shows the extended release of naltrexone over one month trial that indicated the success rate after so many days once an individual has started taking naltrexone.
Clinical Review
More research needs to be conducted regarding the use of naltrexone as an antagonist in addiction recovery. The nature, severity, and duration of naltrexone induced acute opioid withdrawal varies greatly between people and the clinical course of events is unpredictable. With the trend for more addicts to be treated with naltrexone in the community, and the possibility that current addicts may see naltrexone as a misguided means to break the cycle of drug dependence, the potential exists for increasing numbers of similar presentations. Physicians involved in the emergency care of these patients must be aware of the dramatic clinical course of the ingestion of naltrexone in opioid misusers and be prepared to manage the complications.