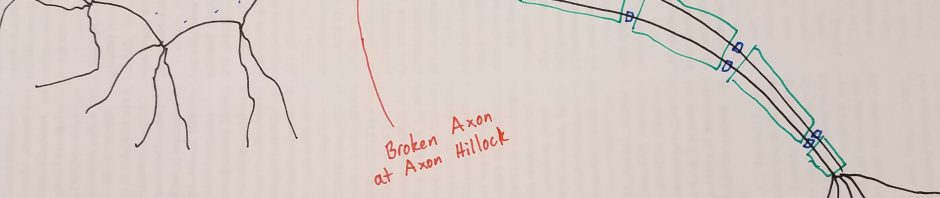
You have probably seen the muscle tremors that affect Parkinson’s patients. Parkinson’s is a disease that kills dopamine-producing neurons in the brain. While traits like intelligence, personality, and memory can decline, the most damage happens to the motor neurons that move our muscles. Over a period of decades, muscle control gradually declines in Parkinson’s patients. There are only a few treatments available for Parkinson’s, and they can only slow the progression of the disease or deal with the symptoms.

So what is actually killing the motor neurons? The cause is still not completely clear, but we know that Lewy Bodies affect the neurons. Lewy Bodies are clumps of sticky protein that build up in the neurons of people with Parkinson’s. Lewy Bodies are also found in other forms of dementia. They are made up of a protein called alpha-synuclein.
And what makes this protein stick together? The answer might be phosphate groups. Phosphate groups are a molecule of phosphoric acid that gets added onto the protein. For some reason, phosphate groups seem to make alpha-synuclein stick together. Maybe it helps the proteins fit together like puzzle pieces. You probably know phosphoric acid from the label on a can of pop. Drinking phosphoric acid in soda is not dangerous (except to your teeth) because it takes special enzymes to add the phosphate groups onto proteins.
Proteins that tack phosphate groups onto other proteins are known as kinases. It turns out that most kinases are controlled by other kinases, so there is a complicated web of on and off switches inside our neurons. If one kinase is mutated, it can affect dozens of other types of kinases, making them sluggish or hyperactive. This can eventually lead to the clumps of neuron-killing protein.
Interestingly, when one piece of a-synuclein gets a phosphate group it encourages other ones to do the same. This makes alpha-synuclein act like a prion disease in Parkinson’s patients. The prion disease of mad cow disease made headlines when the public learned that their beef cows were eating the brains of other cows. That’s a great way to spread a prion disease, and fortunately humans don’t normally swap much brain tissue. But this does explain how muscle problems can start in an arm or leg and spread to the rest of the body, and how dementia can appear in late stages of the disease. Parkinson’s can start in one area of the brain and slowly march across the brain from neuron to neuron.
The tremors of Parkinson’s make it impossible to eat and difficult to sleep. People that work with their hands for a living are affected even more. If we can stop proteins from sticking together in their neurons, we might be able to stop the disease. Unfortunately, the root cause of the phosphorylation of a-synuclein does not just involve one gene. It will take a lot of work by scientists and probably some supercomputers to put the puzzle pieces together so we can take other puzzle pieces apart.
The Stickiness of Parkinson’s Proteins