Think back to your most vivid memory. I would guess you can remember just about every detail about that situation. What time of day it was, where you were, what happened, and how you felt. Chances are, it probably is a stressful memory.

We tend to remember stressful events in great detail but it is probably to our benefit for us to remember some stressful events. Knowing what put you in danger one time will help you to avoid that stressful situation a subsequent time. In fact, when experimental rats were given a substance that decreased their anxiety, they were able to remember less about a stressful situation when put in it again.
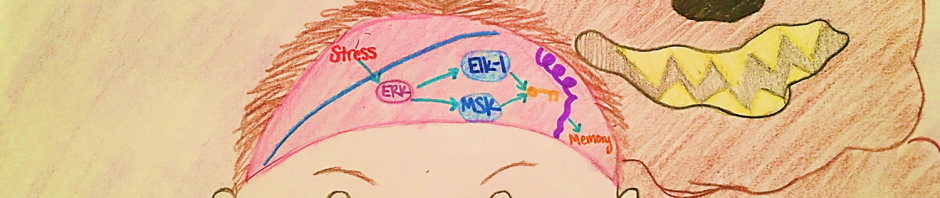
In your brain, there is an area called the hypothalamus, which is vital to forming memories, especially contextual ones, and plays some role in responding to stress. When you’re in a stressful situation, hormones called glucocorticoids are released into particular areas of the hypothalamus. The release of these glucocorticoids is vital for the formation of memories related to stressful situations that may keep us safe. The glucocorticoid release triggers effects in the cell that lead to a change in the shape of our DNA structure that makes it easer to read genes that contribute to memory formation.

That’s all fine and good when it goes right, but what about when it doesn’t? For people with anxiety, the glucocorticoid hormones are released more often and in higher concentrations, leading to stronger memory formations, even in non-stressful situations. These anxious people that are already forming stronger memories are more likely to develop PTSD as a response to events of extreme stress.
The good news is that there are ways to prevent this stressful memory formation. Anti-anxiety drugs like Lorazepam have been shown to reduce anxiety by blocking the changes to DNA structure elicited by stressful situations. Similarly, regular exercise has also been found to inhibit the changes in DNA that lead to stressful memory formation. I’m not suggesting that exercise is the ticket to treating anxiety but it certainly can’t hurt when it is in combination with drug treatment and therapy.

Understanding these molecular markers of anxiety will hopefully help scientists in the future to develop medications that may be more effective in treating anxiety disorders and PTSD. In the meantime, knowing that there are major structural changes to DNA in people with anxiety can help us to be more understanding to those living with anxiety when we are able to realize that they cannot do anything to control this phenomenon from happening.
How Stressful Memories Contribute to Anxiety