Our final neurochemistry topic of the semester focused on the developmental disorder known as autism. Autism is a very interesting topic because its cause can be due to so many different events and it is relatively hard to get a concrete diagnosis. The general definition of autism states that it is a disorder of neural development characterized by impaired social interaction and communication. The paper that we explored outlined two particular hypotheses for the cause of autism, looking at both the genetic factors as well as the possibility of different environmental factors present in the causing of autism.
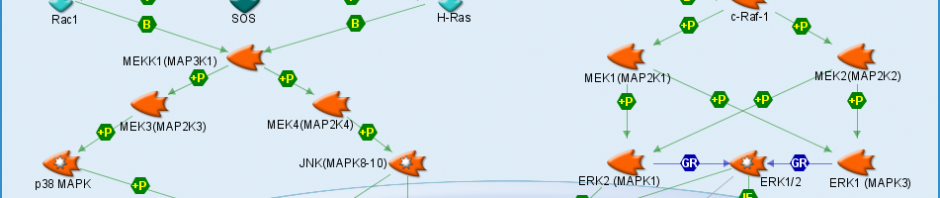
The world that we live in is becoming increasingly complex as science develops new ways to build different products with new materials that often contain both heavy metals and xenobiotics. Xenobiotics are simply chemicals that people can come in contact with and the main heavy metals that our paper focused on were arsenic, lead, and mercury. Combining these heavy metals and xenobiotics with genetic predisposition there is an extreme risk for the development of autism. I will start out by briefly describing the science behind the hypotheses outlining the development of autism. The development of autism starts out with either genetic factors or the exposure to heavy metals and xenobiotics causing impaired sulfur metabolism. This impaired sulfur metabolism then inhibits the activity of methionine synthase causing decreased methylation of DNA, ultimately resulting in developmental delay and autism.
One of the main topics that we talked about in our discussion dealt with diagnosing autism and what this does to the social status of a child. Diagnosing autism can be very difficult because the symptoms can cover a very broad spectrum ranging from very severe to very minor. It is very hard for parents to know when to take their children into the doctor to get examined because it’s hard to know for sure if your child is simply in an awkward stage of development or is in fact suffering from the developmental disorder known as autism.
I personally have a family friend who was diagnosed with Asperger syndrome, which is an autism spectrum disorder that is very similar to autism but can be less severe. In my friend’s case, he had a very awkward childhood and struggled socially prompting his parents to take him to the doctor, ultimately to be diagnosed with Asperger’s. He now has grown up substantially and if you didn’t know that he had been diagnosed it would be impossible to tell that he has an autism spectrum disorder but he will forever have the title of having Asperger’s. This is just one example showing the difficulties of diagnosing autism spectrum disorders and how hard it must be to label a child with autism.
It will be very interesting to see whether or not the number of cases of autism will continue to increase at the rate it is today now that scientists are uncovering more and more information on the causes of autism and whether or not they will be able to come up with a way to either prevent autism or treat individuals that are already suffering form the developmental disorder.
Is the complex world we live in a possible cause of the rising cases of autism?