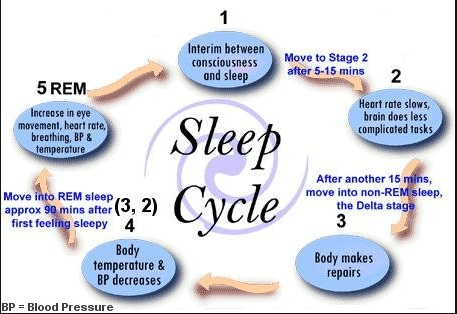
Figure 1: A general picture of lucid dreaming.
Sleep and memory
All through grade school and college, I always heard people say that staying up late cramming before an exam is really counterproductive and shouldn’t be done. I never believed it because I figured the more information I could go over for the exam the better. However, after reading this weeks paper on sleep and memory, it might be time to switch things up.
The paper really focused on the circadian oscillations of cAMP, Ras, MEK, CREB, and MAPK as part of the same signaling pathway. These elements as part of this pathway seem to be downregulated during the day, but are upregulated during REM sleep which is known to have activity in the hippocampus during it. The hippocampus is also known to be a site of memory consolidation, hence the signaling pathway and memory are coupled. For more information on this topic, please see the paper found here. REM sleep is also known to be when people are dreaming. This is where the idea of lucid dreaming comes from.

Figure 2: A personal account of how to lucid dream in a few easy steps.
What is lucid dreaming and how do you do it?
Lucid dreaming is simply a dream where the dreamer knows they are dreaming. Some people use this realization to actually take control of their dreams and determine their outcome. This can be very helpful for people preparing for something like a stressful meeting or public speaking as they can act out these situations in their dream to build up confidence to do it in the real world. It also just offers a fun skill for those who have ever wanted to control their dreams. But how is it done? Well, its not exactly down to a science, but there are a collection of things that one can do to have a better chance at lucid dreaming (coming from people that self report being able to lucid dream). Below is that list of those things which can be found here. Please note that I took some liberties in the names of the steps as well as some of the descriptions.
- Preparing your bedroom
- Do things to induce good sleeping habits. You want to induce REM sleep so do things to get good quality of sleep. Things like blackout curtains and white noise machines to block out ambient light and noise. Try calming techniques before going to bed so you are in a comfortable state first.
- Starting or keeping a dream journal
- This keeps you in tune with your dreams and prevents you from just having dreams and then forgetting.
- Recognize dream themes
- Don’t just write down dreams then forget about them. Review the journal and look for themes. Do certain people or event come up regularly? Try to recognize this in the dream.
- Perform reality checks
- This is a way to recognize if you are in a dream or not. These can be things like trying to push your index finger through the opposite palm with the expectation that it will happen. In a dream you will be able to make it happen! Or you could try looking at your hands and feet, in a dream they tend to be distorted. Finally you can try looking at a clock or book, then quickly looking away, and then looking back. In a dream the time or text will have likely changed but in reality it obviously doesn’t.
- Trick your brain as you fall asleep
- As you drift off to sleep, try repeating a phrase like “I will be aware that I am dreaming.” By repeating this you are essentially tricking your brain to remain aware as you fall asleep.
- Try going back to sleep
- After waking up from a dream, try to fall back asleep while thinking about was happening in the dream, but this time focus on knowing that you were aware it was a dream as you fall back asleep.
- Induce sleep paralysis
- Instead of #6, you can try this alternative method known as “wake induced lucid dreaming.” When your alarm goes off, try to get back to sleep as soon as possible, but keep your mind focused and active to increase the chances of lucid dreaming. However, be warned, my keeping your mind awake while your body falls back to sleep you may induce sleep paralysis which can be very frightening because you are unable to move.
- Wake, Bake, Back to bed
- This involves setting an alarm at some point through the night (typically 4, 5, 6, or 7 hours into sleeping with 6-7 hours to be most effective for most). This increases the chance of waking up during REM sleep and remembering your dream. Then stay awake for 30-60 minutes before going back to bed. The idea is to wake up your brain while your body is still tired.
- Take up gaming
- There are actually studies that show that playing video games leads to better dream memory retention as well as the ability to lucid dream. This follows because video games are typically an immersive experience that you are in control of.
- Try to stay in the dream
- Congratulations! Hopefully by this point you are beginning to lucid dream. However, don’t get frustrated if you can’t do it for very long. It is common for those that are first learning to lucid dream to get so excited when they finally do it that they wake themselves up.
And there you have it! How to lucid dream! The length of the post is a little long, but hopefully you’ll be lucid dreaming in no time with a little practice!
And finally, here is my arstract on how lucid dreaming can make your dreams awesome!




![Best Cannabis Leaf Pictures [HD] | Download Free Images on Unsplash](https://images.unsplash.com/photo-1597266029701-618ac066150a?ixlib=rb-1.2.1&ixid=MnwxMjA3fDB8MHxzZWFyY2h8MXx8Y2FubmFiaXMlMjBsZWFmfGVufDB8fDB8fA%3D%3D&w=1000&q=80)