What is Autism?
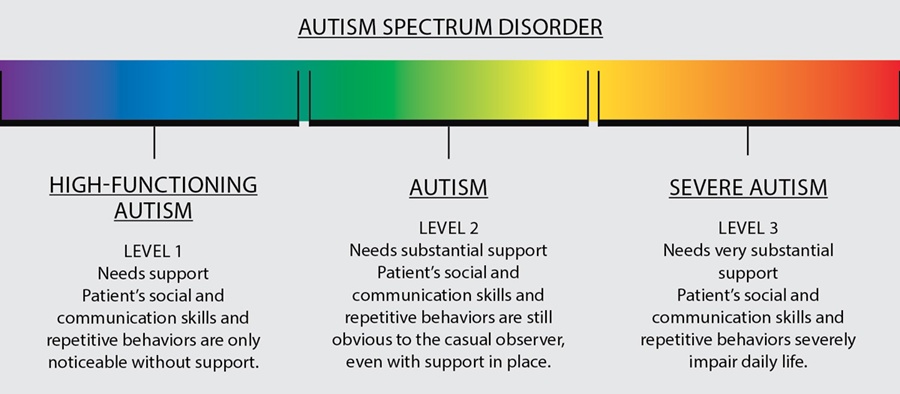
Autism is a developmental disability typically affecting communication and social interaction. Symptoms are usually apparent in the first three years of life. Autism is considered a “spectrum disorder.” This means its symptoms vary from person to person and ranges from mild to severe. There is no given set of characteristics that applies to all individuals with autism. It affects a person’s brain function in differing ways and at varying degrees. Thus, each individual affected with autism is unique in his or her own way. There is no single cause associated with autism; however, research indicates biological or neurological differences in the brain. It is five times more prevalent in males than in females but is not limited to any race, ethnicity, or socio-economic background.
Diagnostic and Statistical Manual of Mental Disorders V Classification of Autism
According to the DSM 5, the term Autism Spectrum Disorders (ASD) is a single umbrella term that encompasses the following subtypes:
-Autism,
-Asperger’s Syndrome (ASP),
-Childhood Disintegrative Disorder(CDD)
-Pervasive Developmental Disorder-Not otherwise specified (PDD-NOS)
It also emphasizes that individuals with ASD must possess symptoms from early childhood even though they may not become apparent until later in life. These diagnostic labels are based on the commonalities and the distinctiveness of the symptoms in each type of ASD. The defining symptom of ASD is substantial deficit in the area of social relations and communication. Asperger’s Syndrome is mostly considered to be a mild form of ASD, and it’s considered to be at the high functioning end of the spectrum. PDD-NOS is commonly used for those individuals that do not fully meet the criteria for ASD or Asperger’s Syndrome. CDD differs from autism in its occurrence as it develops in children with normal development that later start regressing. The ease with which an autistic child learns to socialize depends greatly on his or her communication skills. Parents, teachers, siblings as well as peers play a very important role in fostering life skills required for developing social skills.
Learning with Autism
Teaching social skills one-on-one may not be very effective unless interactions are linked with normal peers. Thus, a natural learning environment plays a pivotal role in nurturing social development in children with autism. At school, they should be encouraged to interact with other students mostly during recess, lunch time, or during special activities such as sports, arts, or drama/music. At home, parents and siblings can work together to provide an autistic child with opportunities for positive social interactions.
What Causes Autism
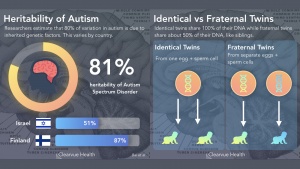
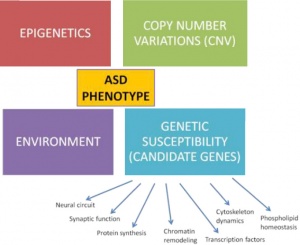
Though there are many different factors that could contribute to autism such as environment, problems during development, and illnesses females may experience during gestation, genetics is going to be mostly focused on here.
Mothers who contain gene variants of ASD are more likely to pass this onto their children. Females are less likely to present signs of ASD and to be a carrier of it. They can carry the same genetic risk factors without the signs of it but if they were to have a male child then that individual is more likely to be diagnosed with ASD after birth. The gene that is most commonly known to cause autism or autism spectrum disorder is fragile X syndrome. All males carry an X and a Y chromosome, and receive the X from their mothers. Females carry two X chromosomes, receiving one from each parent. Hence girls can inherit fragile X from either parent, while boys inherit it only from their mothers. Females are protected from fragile X syndrome to a degree because they have two X chromosomes. Because one of their X chromosomes is most likely to be normal, the effect of the abnormal one is less pronounced, and they usually have milder problems than males, with only 30 percent having intellectual disability and the rest having emotional or learning problems.


:max_bytes(150000):strip_icc()/treatments-for-adults-with-asperger-syndrome-259901-Final-1383adbeffcc4d3a9a2c7020d7bb306d.png)
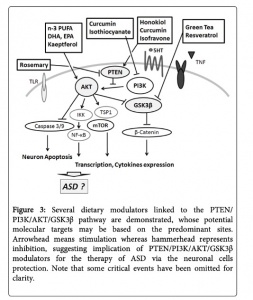
![PDF] Drug therapy in autism: a present and future perspective. | Semantic Scholar](https://d3i71xaburhd42.cloudfront.net/145fda4d09aa46a5e6dc9685253313d808fafb73/5-Figure1-1.png)




 The perfect women would still get all the work done around the house, take care of about 4-6 children, cook food for the whole family (with a dessert – daily), great their husbands nicely dressed and with a smile at the end of the day, then have a long night of sleep. All this, in the midst of the Cold War. Anything seems off? Well, it should, as explained by the perfect recipe of a ‘50s housewife: daily amphetamines and barbiturates.
The perfect women would still get all the work done around the house, take care of about 4-6 children, cook food for the whole family (with a dessert – daily), great their husbands nicely dressed and with a smile at the end of the day, then have a long night of sleep. All this, in the midst of the Cold War. Anything seems off? Well, it should, as explained by the perfect recipe of a ‘50s housewife: daily amphetamines and barbiturates.