Brain games, social activity, constant learning, exercise. Surely, they’re mentally and physically stimulating, not to mention they can be extremely enjoyable. But can a stimulating environment go beyond enjoyment and enter the realm of affecting something like your brain’s ability to combat the tolls of ageing like mental decline or protect itself after injury?
The Effects of Environmental Stimulation
Research in animal studies has shown that mental and physical stimulation can actually play a part in aiding your brain’s protective reserve. There are two types of reserve, cognitive and brain reserve. The two are very similar and intricately linked; cognitive reserve is the brain’s ability to resist and protect against damage while brain reserve is its ability to combat age and disease-related defects. Furthermore, the research has shown that this overall reserve plays an active role in reducing the risk of dementia and slowing the rate of memory decline. Additionally, these types of reserve have been linked to the brain’s capability to repair itself after a trauma.
Find Your Personal Environmental Stimulation
A stimulated environment can look different for everyone. Activities like knitting or board games might stimulate some while boring others, but the premise of stimulating your brain should nonetheless remain generally understood. Given that new research shows environmental stimulation can lead to increasing important brain function, it is arguably important to determine what exactly mentally stimulates you. Mental stimulation can be different from mental enjoyment, however. For example, watching Netflix for hours can be extremely relaxing and enjoyable, but often mindlessly watching television programs necessitates very little mental stimulation. Things like higher learning, attending social events, and playing instruments requires more mental exertion, and life experiences like these are said to grow the brain’s protective reserve. So, finding activities that not only you enjoy but that also cause your brain to “work harder” can prove to satisfy you both regarding entertainment and your long-term mental health.
The Science
Many portions of the brain have shown to be affected by environmental stimulation both at the cellular and molecular level.
At the cellular level: processes like neurogenesis, gliogenesis, angiogenesis, and synaptogenesis are promoted. Neurogenesis is the brain’s ability to produce new neurons from neural stem cells. Support has been shown for its role in the hippocampus of adults to increase the ability to acquire new memories. Gliogenesis is the process that makes glial cells, which include astrocytes, oligodendrocytes, Schwann cells, and microglia. These together play vital roles in regulating neurotransmission, modulating learning and neurogenesis, and providing structural and functional support to neurons. Angiogenesis is the process that develops new blood vessels, which is vital for proper brain function as oxygen and nutrients are required by neural tissue. Lastly, synaptogenesis is the creation of synapse connections between neurons, which is imperative in improving existing connections and making new neuronal connections.
At the molecular level: environmental stimulation can affect both early and late gene expression of the neocortext. This leads to changes in gene transcription that codes for particular proteins involved in neuronal transmission. The two main areas affected are changes in neurotransmitter and neurotrophin activity.
Regarding neurotransmitters: stimulation causes enhanced sensory, cognitive, and motor activity by changes to extracellular neurotransmitters, membrane transporters, and receptor levels many systems (for example, serotonergic and noradrenergic systems).
Regarding neurotrophins: neurotrophins bind to the p75 and Trk trans-membrane receptor proteins and they regulate neuronal development and function. Stimulation can affect the processes they’re involved in, like “cell proliferation and differentiation, axonal and dendritic growth and remodeling, synaptogenesis, and synaptic function and plasticity”. (To read more about this study, click here.)
“Our country is getting bigger and bigger. We were much thinner when I was a kid.”
“Our food is so processed, but fast-food is convenient and much more delicious than healthy eating. Making healthy meals just takes too much time.”
These are just a few comments about today’s American culture regarding food. The problem is-they’re relatively true statements. America is arguably more fast-paced than earlier times and also more productive, but that comes at a cost. Increased productivity can come at the cost of bodily health, which often times means the way people eat can be affected. Fast-food is consequently often consumed to compensate for a lack of time needed to prepare home-cooked meals. In the short term, fast-food is the answer, but the long-term effects of eating it regularly can take a large toll on an individual, and data shows than the American people as a whole have not fared well in the wake of the American fast-food lifestyle.
The Problem
According to the World Health Organization (WHO), fast-food comprises approximately 11% of the average American diet, and this food is largely unhealthy due to added sugars, preservatives, and a lack of natural meats, fruits, and vegetables. (If you want to read more about the WHO’s analysis of eating in America, click here.) This is correlated to the rise in total calorie, meat, and grain consumption, ultimately leading to an increasingly obese society. Increased intake of unhealthy foods almost ensures an increased weight in the U.S. population, but another culprit is responsible, in part, for the rise of obesity: lack of exercise.
Along with an increase in unhealthy eating, Americans are exercising less and less. Whether it be from lack of time, inaccessibility to a workout facility, or an inadequate understanding of the overall benefits that accompany exercise, decreased exercise in America has nonetheless played a role in the rise in obesity trend.
A Solution
Many people are unaware of their options regarding healthy foods or healthy food preparation. Furthermore, many do not know of the true consequences of long-term unhealthy eating. A few of these consequences include: weight gain, high blood pressure and high cholesterol. To combat this, persistent education beginning at a young age should be pursued-a child’s education should include healthy lifestyle awareness as it affects their bodily health long-term. If young children, teenagers, and young adults are ingrained with the skills and knowledge of healthy eating and ways to prepare such food, as well as education on time-management in taking care of your bodily health, the obesity “epidemic” could be challenged.
The Science
Insulin and Leptin are hormones in the body that play a role in proper food intake and energy metabolism. During proper signaling after food intake, insulin and leptin work together to simultaneously inhibit the AgRP neurons while activating the POMC neurons. The increase in POMC neuronal activity in turn activates MC4R neuronal activity that is responsible for satiety and stimulation of energy expenditure. AgRP neurons tell your body to “eat” while POMC neurons tell your body your “full”, so when their inhibited and activated respectively, proper metabolic activity in response to food intake can occur. However, long-term overeating can lead to improper signaling in this pathway. Persistent overeating leads to neuronal inflammation that can lead to resistance of both the AgRP and POMC neurons, so overactivity in the AgRP neurons can continue, which tells your body to continue eating. This a vicious cycle of overeating due to the body’s inability to feel truly “satisfied.” This leads to the increased overall caloric intake and ultimately weight gain.
At what point is someone addicted to drugs no longer capable of making the decision to continue using drugs? At what point does the long-term effect of using drugs affect the brain in such a way that it is virtually impossible to stop using drugs on your own? This is a topic that continues to be debated among both the scientific and legal communities.
Common Convention vs. A New Proposal
Currently, addicts can be held responsible for any action they take however under the influence they may be, or how far into their addiction they are. Although they are not entirely in control of their actions due to the change in their neurochemistry, the law states they are responsible for any actions that are a result of the initial decision to take drugs. So, what should be done if at some point, people are no longer physically able to make decisions for themselves other than to feed their addiction? One possible answer: change the way anti-drug campaigns are aimed at children and young teenagers.
Anti-drug campaigns traditionally have been centered around making drugs and alcohol seem as scary and unhealthy as possible. These campaigns are aimed at middle school kids who have very little prior knowledge Now although that is true, one could argue that this approach is dangerously misleading. Long-term, hard drug use can lead to extreme health decline and a loss of decision making regarding using the drugs, but this isn’t so apparent after the first use of a given hard drug. What most anti-drug campaigns don’t tell you is the reason they are so addictive is because they do give you an immediate, rewarding feeling known as a “high.” Being open and honest about this when talking about drugs could be crucial because after a kid uses for the first time and only sees the immediate pay off, they might begin to think that they were misled and that drugs truly couldn’t be that bad.
There is a happy medium between showing kids horrifying pictures of hard-core drug abuse and telling kids that drugs are as rewarding as they are rumored to be. Laying out the facts and being as honest as possible while maintaining the agenda of preventing drug abuse is a viable option.
The facts are
Drugs do give the immediate “high” that can be very rewarding, but it is a slippery slope since most addicts don’t realize they’re addicted till it is too late
Socially, drug users are outcasts, and being dependent on hard-core drugs makes holding down a proper job and living situation very difficult
Hard-core drug use cannot last before major medical problems occur
Before, kids were just told drugs and alcohol are bad for you and that they should just stay away. “Trust us,” with “us” being law enforcement. And even though it is true, telling kids to simply “not do drugs” glosses over the real, addictive powers of drugs.
The Science
Cocaine or methamphetamines cause a rapid increase of dopamine that is released in the ventral tegmental area (VTA), nucleus accumbens (NA) and prefrontal cortex. These drugs are so addictive because they don’t allow for the reuptake of dopamine due to their strong binding to the dopamine-reuptake transporters. This blocking effect, which causes a long-lasting high concentration of dopamine in the synapse which go on to affect adjacent neurons, is the source of the notorious “high” feeling associated with taking cocaine and methamphetamines. Additionally, amphetamines cause the phosphorylation of cAMP response element-binding protein which goes on to affect synaptic plasticity and aide in creating the overall addictive behavior.
I was four years old when I remember standing on the upstairs landing of my childhood home staring down at two strange men. With my stuffed bunny in hand, I frantically looked for my mom while on the verge of tears. I was scared I had “lost” my mom, when just then she came walking in the front door as if nothing was wrong, because in fact nothing was wrong. These men were here remodeling our kitchen, and I was safe as could be.
I had always wondered why that memory was so firmly stuck in my brain. I remember what I was wearing, how sunny it was, and how the men tried to reassure me my mom was just outside doing yard work. But the formation of that very distinct memory was more than likely due to the immense stress the four-year-old me experienced. Not all memories are formed the same, with some being strongly formed, even to the point of having a negative effect.
The Science of Making Memories
Strong memories can be made, occasionally during devastating experiences, and sometimes result in the development of stress-related disorders like major depressive disorder, anxiety, and post-traumatic stress disorder. In fact, 10-20% of those who experience traumatic events develop some type of these disorders. This mystery is being pursued fervently, with some important headway being made.
In a study performed by Johannes M. H. M. Reul, the formation of memories related to stress events was analyzed in the use of animal models where the forced swim test was applied. The premise of the test is to place rats and/or mice in water and observe the length of time it takes for them to abandon struggling and opt to float to conserve energy. After some time, they placed them back in the water and found that on average it took less time for the rats and/or mice to begin floating, showing an “enhanced behavioral immobility behavior,” which is based on the formation of the memory during that stressful initial forced swimming experience. The molecular changes and processes of these rats and/or mice gave rise to interesting results.
Stress evokes glucocorticoid hormones, or corticosterones in rats and mice, which strengthen the consolidation of memory formation via activation of glucocorticoid receptors (GR). Additionally, glutamate is released following stressful events, and it goes on to activate the NMDAR-ERK-MAPK pathway. Both the GR and NMDAR-ERK-MAPK pathways work in tandem to facilitate the activation of kinases MSK1/2 and Elk-1. This results in the acetylation of histone H3 (H3S10p-K14ac), leading to the transcription of genes like c-fos and egr1, which are immediate-early genes. The induction of the transcription of these genes is essential in the consolidation of memory formation.
A Reality of PTSD in Today’s Society
When people think of strong memories being made that result in stress-related disorders, what commonly comes to mind is soldiers experiencing PTSD at the hands of deployment, and justifiably so. Our veterans are subject to extremely stressful experiences, like front-line combat, the loss of fellow soldiers, sexual assault or harassment, and countless more.
Figure 1. Taken from VA.org – it depicts a soldier who has an experience with PTSD.1
As a result of any given war where the U.S. has been a contributor, a large number of veterans have experienced PTSD. The U.S. Department of Veterans Affairs provides astonishing information about veterans and PTSD, including:
11-20% of veterans of Operations Iraqi Freedom (OIF) and Enduring Freedom (OEF) developed PTSD.2
12% of veterans of the Gulf War have PTSD.2
15% of veterans of the Vietnam War were diagnosed with PTSD during the war, while an estimated 30% of the war’s veterans have had PTSD within their lifetime.2
While research is ongoing in the incurrence and treatment of PTSD in general, the reality of millions of people today is a life living with PTSD.
There is a question that appears on every course evaluation at the end of the semester: this course improved my ability to connect between this area and other areas of study. Saying that this course improved my ability to do this is an understatement, but that is why I love liberal arts learning in the first place.
One of the reasons I chose Concordia was because I wanted to connect science to other fields of study. I wanted to see how we go from tiny cells to complex beings. I figured a liberal arts educations would help me see that. This course really helped me see that. A prime example of this came during the week we discussed the neurological mechanisms of overeating. Overeating, in my opinion, is not always the fault of the individual, but rather larger social forces that dictate what sort of foods are available. The paper showed that it was also a brain disorder. Reading this paper, I was able to connect information I had learned in my sociology class with information in my neuroscience coursework. It was amazing to see the effect that societal structure had on the brain. I realized how complex society really is, which is a major part of Concordia’s BREW and liberal learning. BREW stands for becoming responsibly engaged in the world and in order to do so it is my responsibility to understand the world’s complexities.
I have always prided myself on my ability to explain things. I was told early on in my college career that if I cannot explain the material, I are learning to a non-science major, then I do not know it well enough. This influenced how I studied. But when I got to this class, I was not discussing what I learned with non-science majors. I was discussing things with science majors, senior science majors no less! Suddenly, I was not the best explainer in the room. I was alright at explaining the simpler concepts, but the oral exams and the speed discussion Wednesdays quickly made me realize that I needed to adapt to my audience. From there things changed, I started doing more research for my Wednesday topic and my blogs became more detailed. My improvement showed. I was better able to participate in both Wednesday and Friday discussions. Dr. Mach even complimented me on my improvement. I felt confident.
Additionally, this course improved my ability to explain things to a non-science major. The blogs forced me to really think about what a non-science major would now. The articles summarized in the blogs were often very dense and hard to summarize. I had to choose what background information to summarize and what information I should ask my readers to find at a link. I also had to determine what information from the article to put in the blog. A full summary of the article would not be interesting to read. Some information had to be omitted. Through this course, I improved my ability to analyze my audience. I learned how to explain information to scientists and non-scientists and when to switch between the two.
The skills I learned in this course will greatly help me after college. I plan on going to medical school and becoming a doctor. As a doctor, I will have to explain scientific concepts to non-scientists. I need to convey information in a way that they will understand, conveys a point, and is respectful of them. The blogs and discussions allowed me to see connections between neuroscience and the social sciences, making me able to be more understanding and respectful. I am also able to better determine what a person needs to know.
Though medical school is my first choice, I still love research and science itself. As a scientist, I need to explain data to other scientists. I need to have the tone and word choice of a scientist. I must be able to read, speak, and write science. The blogs and discussion made me better able to do this. I feel more confident in my ability to this. I feel like a scientist!
As a kid, recess is one of the best parts of the day, just a half hour to run around and do whatever. There were slides to slide down, things to climb, and games to play. It is a time when a kid can do whatever he or she wants. As fun as it, recess serves an important purpose. It not only fosters social development, but brain development. Physical activity and enrichment promote the development of new connections, aiding learning.
But this need for enrichment does not stop with childhood. The adult brain is remarkably flexible. However, the discovery of enrichment’s role is one of the most recent developments in neuroscience, so it is still unclear how exactly this development works or how flexible the adult brain is. Still, there is some benefit.
Enrichment
Enrichment affects the brain at both the cellular and molecular level. At the cellular level, it affects the brain in four different ways.
First, enrichment leads to a process called neurogenesis. This is exactly what it sounds like, the development of new neurons. More specifically, enrichment leads to the development of new neurons within the hippocampus. This brain structure helps integrate memories, making it easier to form new ones.
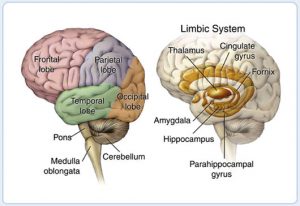
The second effect enrichment has is called gliogenesis. This is an increase in the glia cells, non-neuron cells that aid in neuronal function. These cells perform a wide variety of functions. (For a summary, click here). Forming new glial cells helps both new and existing neurons perform better. As with neurogenesis, enrichment forms new glial cells in the hippocampus. Glial cells are also formed in the neocortex, the outer region of the brain that is responsible for processing information. The neocortex is divided into four different lobes (seen in the figure below[i])
. These lobes connect with each other, which is how people process information. Increasing the glial cells improves the connections between these lobes, allowing for more efficient processing of information.
The third effect, angiogenesis is not very well understood. Basically, it is improved blood circulation and nutrition to a certain area. In this case, enrichment leads to improved blood flow to the hippocampus and neocortex. Interestingly enough enrichment may have no effect on angiogenesis. It may be caused by physical activity alone.
Finally, enrichment causes synaptogenesis. The synapse is the gap between two neurons. It is the base for all interneural communication. Creating new synapses allows a neuron to connect with more neurons. It is sort of like discovering Google for the first time. Forming these new connections is how people learn. Like angiogenesis, it is still unclear what role enrichment has in synaptogenesis. It may have no role. Some studies have suggested that physical activity alone may be the cause of synaptogenesis.
Enrichment also affects neurons at the molecular level. It affects gene expression, neurotransmitters, and neurotropins.
Enrichment changes what genes get transcribed. This determines what proteins a nerve cell makes and what it can do. Enrichment promotes transcription of genes that improve learning and memory. Essentially, making an environment exciting enables further learning. Learning begets learning.
The exact effect of enrichment on neurotransmitters is unclear. Studies have failed to find any changes in base levels of acetylcholine, glutamate, and GABA. However, some studies have seen an increase AMPA and NMDA receptors. These receptors are critical in long term activation, a process that essentially makes a neuron more responsive. However, not all studies found the same result.
Lastly, enrichment also affects neurotrophins. These important proteins foster neuronal growth and development. Enrichment has been shown to increase levels of neurotrophins in the hippocampus, neocortex, frontal lobe, and cerebellum. Like angiogenesis, there is still debate on what role enrichment plays. Some studies suggest physical activity alone may be the cause of the increase.
What does this mean?
This information is very new. The experiments highlighting this phenomenon were not and cannot be done on humans. It is not only unclear what role enrichment plays in an animal’s life, let alone a human’s.
Still, there is a lot of hope that comes from this information. Enrichment may play a role in preventing pathological neurological disorders like Alzheimer’s and Parkinson’s. It may even give people with neurological disorders a treatment that does not involve medication. Enrichment could give people a sense of control.
As for people without these disorders, enrichment and physical activity can still be beneficial. It can lead to improved memory and cognitive processing. What exactly this enrichment looks like is vague and debatable. The rats in these studies are given lots of social interaction and toys to play with, things to climb on. It is almost like recess, but what does recess look like as an adult? Well that, dear reader, is up to you.
My capstone course, Neurochemistry 475, truly encapsulated what it means to become responsibly engaged in our world. The course has the same name as the degree I will obtain in May of 2020, so it feels only fitting that the expansive topics I have learned about and experienced this semester through this course, from intracellular signaling to community action, have informed my student life and my citizen of the world life.
I can confidently say that this was my favourite course taken at Concordia. The perfect complement to my last year, this capstone course brought together all of my favourite things about studying science and allowed me to take them into the real world and apply them to the broader everyday life situation.
Neurochemistry 475 was at its heart (at its nerves?) a journal club. Each Monday, we met to discuss a paper we had read over the weekend about a myriad of neuroscientific topics. Throughout the semester, we looked at Alzheimer’s Disease, schizophrenia, obesity, addiction, concussion, cannabinoids, and the brain reserve among other experiences to try and understand more about what happens in our brains. While the topic each week changed, the general story of molecular and chemical signaling remained surprisingly congruent, with the same major players showing up again and again. Some of these are proteins, transcription factors, or second messengers that seem to be everywhere in cellular signaling. Often, something found to be dysregulated in one disease would also be implicated in another experience (one fascinating example of this is Alzheimer’s Disease and Type 2 Diabetes and the story of insulin hormone resistance in the brain). This interconnectedness between the neuron and human experience has shown to manifest in a great number of ways, but grand themes remain constant.
On Fridays, we met outside of the classroom for lengthy, stimulating, and at times heated discussions about that week’s topic. Even though we met at 8 in the morning, this was my favourite class of each week for the semester! After the in depth analysis and critical investigation of the molecular and chemical signaling pathways that we began earlier in the week, on Fridays we broadened our neurochemical conversation to include environmental and societal implications and factors that can impact someone’s experience. For example, when we talked about schizophrenia, we explored the underrepresentated and underheard voice of women in the medical field, as both medical professionals and patients, to understand why men are diagnosed with schizophrenia (not to mention any other mental health disorder) so much earlier in life than women. In our discussion about cannabinoid reception, we considered the racial undercurrent fueling the War on Drugs and how people of colour are more harshly stigmatized to have drug problems and more violently sentenced with drug (specifically marijuana) related offenses. Friday discussions allowed for the integration of tiny, molecular and neural network ideas with expansive, global network issues and experiences.
Neurochemistry 475 provided the much needed open and encouraging atmosphere with which to bring difficult topics like race, gender, religion, and sexuality into the conversation about the network of electrical and chemical impulses in our brains that ultimately are formed by and inform our experience. Neurochemistry 475 embodies the spirit of liberal learning by exploring the similarities that occur within and between neural diseases and disorders, the life factors that impact these experiences, and the interconnectedness by which all of us live.
After months of chipping away at articles, scaling pages upon pages of reading, and summiting the art of blogging, I’d finally made it to Finals Week, marking not only a culmination of learned skills and knowledge, but also what would be my final fall semester at Concordia College. Getting nearer to the top of this liberal educational mountain, things got harsher and more stressful – battling 10-page papers, running through my medical school paperwork, finalizing final presentations, and of course strenuously studying for the hardest tests of the semester. Through it all, I found myself asking. What was the point of all this? Why am I expending my effort on all this work? Will medical school be 10x worse? But after making it through the storm and reaching the peak, it was clear to see beyond the paper-and-pencil work and understand why the view was worth the fight – looking back at everything I’d done to get there, everything I’ve learned, and seeing where all that hard work has gone. On that note, the stopping point of this hike also marks the end of my time in Neurochemistry. But truly, there’s no better class to reflect on this semester’s educational journey than this unique experience of a course.
If you’re familiar with Concordia’s education at all, you’ll know that the Cobbers are keen on their acronyms. BREW. PEAK. They might be silly, cheesy, and fun terms to throw around, but why does the college keep emphasizing their importance, and what in the world do they have to do with Neurochemistry? To begin, BREWing means Becoming Responsibly Engaged in the World. The ultimate goal of Concordia’s liberal education is to prepare us not only for graduation, but for graduation as adults ready to make meaningful impacts in the community around us, wherever that community may be. The task of turning a bunch of fresh-out-of-high school students into critically thinking and responsible adults in 4 or less years seems like a daunting task, but that’s why the college instilled 5 main goals for their liberal learning curriculum:
Instill a love for learning
Develop foundational skills and transferable intellectual capacities
Develop an understanding of disciplinary, interdisciplinary and intercultural perspectives and their connections
Cultivate an examined cultural, ethical, physical and spiritual self-understanding
Encourage responsible participation in the world
I won’t lie – at a first glance, a 400 level science course with a name like ‘Neurochemistry’ seemed like anything but a course that would accomplish all the goals above. I didn’t know what to expect when I sat down with the syllabus the first day of class. From my former experiences in neuroscience and chemistry (granted both subjects I do enjoy studying), I could only infer that the course was going to involve lots of memorization, technical writing, and, well, learning pure science. But little did I know I was in for one the most non-classroom-like classes I’d be taking in college, and it certainly has fulfilled many of these goals for me.
What and How Have I Learned?
Piecing together knowledge – letting ideas and learning flow together
At the core, neurochemistry is a science, so there was still some typical “memorize and copy” learning involved – knowing what RTKs are, what kind of GPCR does what, and what second messengers do for your brain. But the shocking thing is, like many of Concordia’s other courses, this kind of rote memorization was kept to a minimum. Sure, we read papers and wrote pieces each week, and we did have tests in the classroom. But the difference came in what we did with knowledge from the papers, the kinds of pieces we wrote, and how we had to express our ideas during tests. Above all, I think, the in-class portion of this course has taught me to collaborate, think critically, learn creatively, and express knowledge and ideas uniquely. When we read the week’s paper, we were not expected to come with every detail memorized, every graph copied, and enzyme listed. Rather, we’d gather together as a class and compile each student’s key takeaways, ultimately trying to make something out of it. We’d think critically about how each piece fit together, and through this collaboration our class would get an actual understanding of the science behind the paper. Furthermore, each of us got the chance to express what we learned on a class wiki page, and we’d also get to do so creatively and artfully (I mean seriously, check out some of our class “artsracts”) by writing our very own Cobbers on the Brain blog posts.
One thing this class has definitely taught me is the capacity to learn from others; to always have a questioning and curious attitude. For the rest of the week, our class would hold one-on-one (speed-date style) discussions about the topic, and each Friday we’d get into two big groups to discuss quite literally anything we wanted to (no, not limited to the scientific parts) about it. These included real issues regarding our topic and the world outside Concordia, society, social problems, the community, and the world as a whole. Each of us had the chance to develop our listening skills by hearing our fellow classmates voice their ideas and thoughts, as well as form our own opinions about such broad subjects. At the end of the week, we’d put our words on a page in blog format, and I definitely enjoyed seeing how each of my classmates expressed their thoughts so uniquely, with different voices and writing styles! This is not to mention the interdisciplinary perspectives and various worldly experiences our BREWing pot (couldn’t help it) of students brought to the table – our class consisted of psychology, chemistry, neuroscience, and students of all different kinds of majors and paths.
As for busy work and tests? Pfft. Never once did we have a “rehearse and regurgitate” style paper or exam. Rather, the “exams” more like fun puzzles to complete and discuss in class from what we’d learned over the course of several discussions – putting together a few pieces of given information by making our very own hypotheses, and ultimately expressing the critical thinking we had developed. It made learning fun, and it made me love what I learned.
What Kind of Skills Have I Learned – How Will They Help me in the Future?
As I head off to medical school next year, there’s the obvious benefits. More knowledge = easier time with some of those dreaded Year One courses. Critical thinking and analysis skills? In the bank. Alas, I could talk about the information, critical thinking, and creative leaning I got from Neurochemistry for hours. But perhaps one of the most unique features of this class was how it combined community service and the hard sciences into one in-and-out-of-class experience, thus labelling it as one of Concordia’s PEAK courses.
The other key component of Neurochemistry was what Cobberville calls a Pivotal Experience in Applied Learning, aptly known as a PEAK. As part of our class, we formed a small group and collaborated with students totally outside most of our disciplines – Social Work students (from all the way across the Bell Tower, in good Ol’ Main) – to create a community service project. Together we had the opportunity to do something, to BREW. The communication and collaboration required to get the project across was immense, and the process was fascinating. In summary, our group aimed to focus on Mental Health in the area. We had to conduct a needs assessment, determine a target population, do something, and evaluate its success. The community and collaboration skills I learned from my other experiences at Concordia definitely helped me on this leg of the trail. Ultimately, we uncovered a massive need (the prevalence of anxiety and depression in young and college-age adults) and were able to raise awareness, help break the stigma surrounding, and bring attention to resources for and around mental health problems to one of Concordia’s most vulnerable populations – first year students.
It’s a difficult climb, but it’s worth it!
That’s not to say the process went smoothly. The hike up this part of the mountain had its own obstacles – needs-assessment partners who didn’t send replies, schools who rejected our project, seemingly countless changes to our original plan, and first year students who didn’t know much about the physiology of mental health. But it’s this whole experience that allowed us to develop our listening and collaboration, work on setting new goals and objectives, and ultimately be adaptable and plastic – just like neuronal synapses – to break unexpected boulders in the way. Like many things in life, communication was key. Not only did we learn to communicate with major community organizations and handle rejection from some, but we also learned to put our knowledge into a format that would be appealing, memorable, and understandable to first-years. No doubt, this part of the journey was beautiful, difficult, but also definitely pivotal.
As for me, will this help my journey into the realm of medical school, and eventually the hospital? The short answer is yes – the same skills I mentioned above are largely parallel to those a doctor needs when working with other doctors, staff, and perhaps most importantly, their patient population.
What Does Liberal Arts Education Mean to Me, and Have I Improved Myself?
For the long road ahead
Right now is the best time to create your tomorrow – Ken Poirot
But did I, after my tiresome semester’s trek up the liberal education summit this semester, BREW? Did I PEAK? Even outside of Neurochemistry and speaking to my 3 years of college here, was all that hustle and bustle during finals week, all those papers, and the entire academic hike worth it? That’s a most definite yes to all those questions. Concordia’s education has definitely prepared me for this year’s culmination in learning, and Neurochemistry was an amazing way to combine all I had learned beforehand. Sure, it was hard, and at times tedious, painstaking work to get to this point. But the invaluable skills and lifelong knowledge I obtained throughout the process will stick with me beyond graduation, as I go out there and become a responsible adult, ready to engage in the affairs of the world.
And that, I believe, is what liberal arts education should do. It’s not just simply memorization and straightforward, linear learning. Even if it does include 10 page papers and difficult exams, or creative community collaborations like in Neurochemistry, it comes down to putting in the extra effort and applying outside knowledge to make sure you love what you learn from them, to develop your foundational skills, and to cultivate perspective, self-understanding, and responsibility. Afterall, without the skills I’ve learned climbing Concordia’s difficult liberal education mountain, I probably would not be volunteering in the community, setting scary big educational goals, and making time for other activities as I go on to complete my final semester of college. Who knows, I might not have reached my goal of getting into medical school either.
So reaching the Top? It’s really only reaching the Start. There’s a whole mountain range to explore out there, and with medical school starting soon for me, the journey is only beginning. But whatever your discipline, your major, or your specialization, your own journey up the education mountain won’t (and should never) stop. And the foundational skills learned from a liberal arts education, and through experiences such as those in Neurochemistry, will serve as the tent to fall into when the going gets seemingly too rough. Oh, what’s that? I see another mountain to climb nearby! So without further aBREW…
The importance of brain health is not all in your head. In fact, there are many ways to boost brain health and to acquire cognitive reserve. First, let’s define what exactly is cognitive deserve.
Cognitive Reserve contributes to preserve function in the face of brain injury and decline. It refers to the ability to make flexible and efficient use of available brain reserve in performing tasks.
Wait… Brain Reserve? What is Brain Reserve?
Brain Reserve contributes independently from cognitive reserve. It is connected to brain features, such as number of neurons and synapses. However, brain reserve also involves a deeper understanding and looks at both molecular and supramolecular biological factors.
How do these relate you may wonder…
Cognitive Reserve refers to the ability to make flexible and efficient use of available Brain Reserve in performing tasks. When brain reserve is enhanced, cognitive reserve will also be enhanced and an increase in the following may be noticed:
Neurogenesis: the generation of new neurons allowing for enhancement of communication between areas in the brain
Gliogenesis: the production of glial cells, such as astroctyes to provide structural and functional support to neurons, or oligodendrocytes to regulate neurotransmission along myelinated axons
Angiogenesis: the development of new blood vessels to provide a healthier vasculature that supplies oxygen and nutrients to the neural tissue
Synaptogenesis: the formation of synapses between neurons allowing for modification and refining of pre-existing neural circuits and improvement of neuronal connectivity
A number of factors can be responsible for these changes at the cellular level. All of which involve an enriched environment that engages our brain.
Mental Exercises: Mental fitness activities, such as a crossword puzzle or a game of scrabble, can help lead to build new neural connections in the brain and improve cell function. As we age, taking part in mental exercises can act as a way to enhance cognitive reserve because of its impact on maintaining brain function. Using a combination of learning new things, problem solving, and recall of long term interactions can be crucial in acquiring cognitive reserve. Continual mental exercises will strengthen our brain, thus increasing neurogenesis, gliogenesis, and synaptogenesis.
Healthy Diet: A healthy diet, such as a high adherence to a Mediterranean diet or dietary intake of antioxidants and omega-3 polyunsaturated fatty acids, have been connected to an increase in cognitive reserve and a decreased risk of developing dementia. Hippocampal neurogenesis has been shown to be modulated by manipulating calorie intake, meal frequency, meal texture, and meal content. Overall, a healthy diet can be a factor of an enriched environment. Thus, eating healthy can positively impact cognitive reserve by playing a role in neurogenesis, angiogenesis, gliogenesis, and synaptogenesis.
Being Active: Similar to a healthy diet, physical activity has been shown to increase cognitive reserve and decrease the risk of dementia. Physical activity has also been shown to affect neurogenesis through increasing cell proliferation and cell survival. Physical activity increases gliogenesis in the neocortex and hippocampus. This gives reason to believe being activity can play an important role in memory consolidation. Finally, physical activity has been shown to increase total dendritic complexity and spine density.
Along with performing mental exercises, eating healthy, and being active, we can also acquire cognitive reserve by being safe and decreasing the risk of head injuries, steadying our nerves, and respecting our bodies. We are all aging. Many of us do not like to think about it. However, we can make the aging process much easier by practicing these effective solutions. Acquiring cognitive reserve can start now and a healthy brain will lead you on path to live a happy life!
For more information on how these solutions can lead to cognitive reserve, follow:
As a December graduate, this is my last college assignment ever. It feels strange writing that. It also feels strange thinking about how I won’t be back next semester. Knowing that, I have started to reflect on my time in college. Did I do everything I wanted to do? Did I live up to Concordia’s ideas? Did I BREW?
I believe I did. I feel like I now have a love for learning. I’ve developed foundational skills. I understand perspectives in not only my discipline but others as well. I have a better understanding of who I am as a person.
Neurochemistry was the last class I needed to complete my Neuroscience major. It was my Capstone. Because of that, I knew it might be a challenging course. I figured I would struggle a lot and would end up hating the class. That wasn’t the case. I actually really enjoyed neurochemistry. I thought the set-up of the class, being almost entirely discussion, wouldn’t be beneficial to my learning. Turns out I was wrong. Having to read different journal articles each week and discuss them throughout the week caused me to think in a different way than I normally did. This type of structure caused me to think more critically. I had to not only try to understand what was going on in the papers, but also make connections to other things I learned in both this class and other classes.
This course was very reading intensive. Every week there was a new scientific journal article to read. This helped me sharpen my journal-reading skills and prepare me for my future. Going into the research field, I will definitely need to know how to effectively read a scientific journal article and make connections to what I already know and to my research. Having to write weekly blog posts will also help me in my future career as a researcher. The blog posts forced me to not only dig deep into what I was reading, but I also learned how to turn my complex thoughts about the articles into concise, easily readable sentences.
If I was to highlight a skill that I have improved upon this semester, even just a little bit, it would be leadership. I am a naturally quiet and shy person. I’ve never thought of myself as a leader. This semester, in this class specifically, I believe I have improved that skill. This semester I was required to lead discussions twice and had to talk about a specific topic that only I had researched at least once every week.
I don’t think a course like this would be offered at a non-liberal arts school. That is what’s great about Concordia. It is a liberal arts college. Learning at a liberal arts school has taught me how to think about the big picture. It has taught me how to think about others and how my actions impact them. It has taught me how to make connections, not only in academics, but in social networks as well.
I believe I have BREW-ed. I have become responsibly engaged in the world. I have a better understanding of not only the world around me, but also myself.
Thank you, Concordia staff and fellow Cobbers, it was a great three and half years.