What is Addiction?
Addiction is a psychology and physical inability to stop consuming a drug, activity or substance, despite it causing physical and psychological harm. People can be addicted to a number of different things, but I would like to focus on drug addiction. Addiction manifests itself in physical and psychological symptoms. Tolerance is related to physical addictions. Tolerance occurs when the body begins to get used to the drug of abuse and effects of the drug are not as strong as they once were. This is why drug users will say that they never reach the level of their first high again.
Psychological addiction manifests in withdrawals and cravings. Withdrawal has physical symptoms including agitation, insomnia, muscle tension, and vomiting. The underlying cause of withdrawal is psychological. Tolerance makes the body dependent on drug use to achieve normal levels of neurotransmitters. When that drug is not used, levels are much lower than they would normally be, leading to physical symptoms. Cravings are the body’s desire for the drug. This leads to desire to use the drug again and is the major culprit in relapse. https://emeraldcoastjourneypure.com/physical-vs-psychological-addiction/
Hijacking the Reward System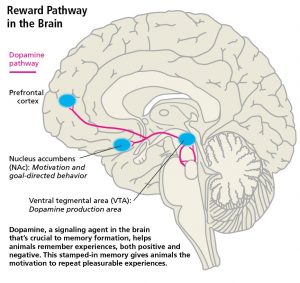
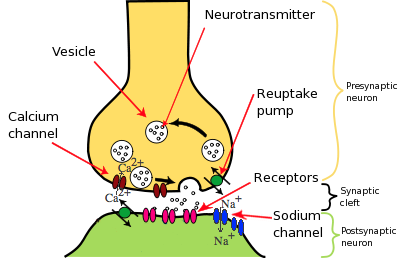
Drugs of addiction directly or indirectly affect levels of dopamine in the brain. The reward pathway in the brain relies on dopaminergic projections between two brain areas, known as the nucleus accumbens and the ventral tegmental area. Shown in the photo on the left. In normal circumstances this is good. The reward pathway allows us to feel good when we eat, drink, or have sex. Drugs of abuse also trigger this pathway by increasing the amount of available dopamine through inhibiting reuptake or enhancing release into the synapse. That is why drug use feels good. This is also why people who are trying to quit using drugs feel so awful during this experience because their body has started to produce less dopamine to compensate for the boost from the drug use. This means that when that boost isn’t happening things that should be naturally reinforcing aren’t. https://www.sciencedirect.com/science/article/pii/S0092867415009629
https://forensicpsychologist.blogspot.com/
Addiction and Learning
Synaptic plasticity is of crucial importance to normal brain function. Synaptic plasticity is the brain’s way of strengthening connections that are used frequently and getting rid of ones that are no longer needed, like the plot of the book you were forced to read in fifth grade. The following video does a good job of explaining what is going on in the brain during synaptic plasticity.
As mentioned earlier, drugs of abuse cause an increase of dopamine at the synapse. This excess dopamine. One of the receptors that dopamine binds to causes AMPA receptors to allow more glutamate in or can stimulate the release of more glutamate into the synapse. This means that more LTP takes place.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3280337
https://schoolbag.info/biology/living/230.html
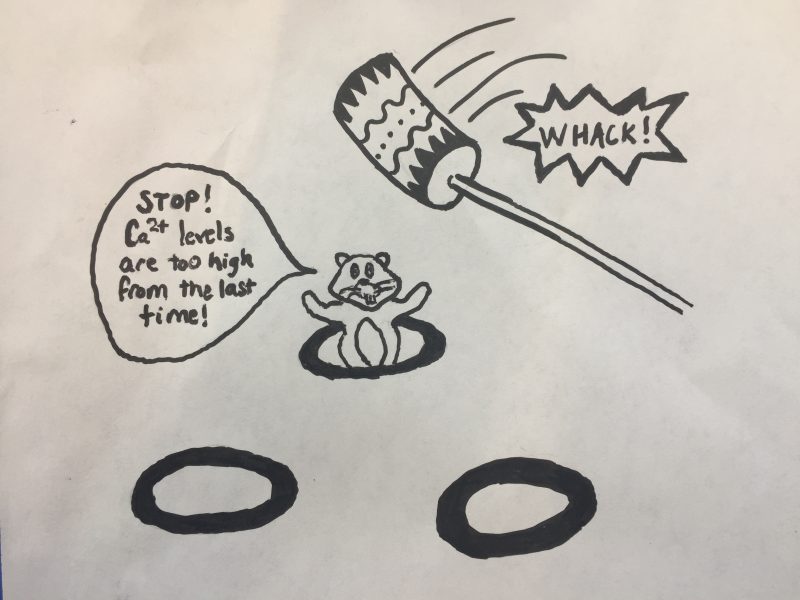
The graphic above gives a good representation of what happens in the brain when drug addiction occurs. Two things happen when in regards to synaptic plasticity when drug use occurs. One is that initial drug use causes a strengthening of the connection between the drug use and the reward pathway. After continued drug use, AMPA receptors are removed from the synapse. This means more drug use is needed to achieve the same amount of stimulation that exists in someone who has never used drugs. The brain knows there is a connection between the use of the drug and an increase in dopamine and glutamate levels and this can lead to drug-seeking behaviors.
A Glimmer of Hope: Addiction Treatment
Addiction changes connections in the brain. This shows why it can be so hard for people to quit. The bright side is that there are a lot of treatment options out there for people who want to quit.
Medications can be used but are typically used in conjunction with another treatment option. The medications are meant to make the transition off drugs easier. They can curb some of the cravings which make people less likely to relapse. They can also curb some of the nasty symptoms that come with withdrawal. Medications are also helpful when people have a co-occurring mental illness that the drugs were being used to manage the symptoms of.
Therapy can also be used to treat addiction and can happen in either an inpatient or outpatient setting. Therapies are meant to change thoughts about drug use and increase life skills, such as coping. Therapy can also be used to treat co-occurring mental health conditions. Therapy can be used successfully in maintaining sobriety.
https://www.drugabuse.gov/publications/drugfacts/treatment-approaches-drug-addiction

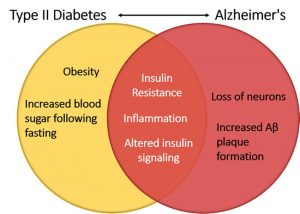 ://www.researchgate.net/figure/Insulin-signaling-linking-Type-II-diabetes-and-Alzheimers-disease-Alterations-in_fig4_323247347
://www.researchgate.net/figure/Insulin-signaling-linking-Type-II-diabetes-and-Alzheimers-disease-Alterations-in_fig4_323247347