When we hear the word “autism,” there are likely several things that come to mind. For many, it’s likely the image of the stereotypical “gifted” child – a child who often talks obsessively about unusual subjects, speaks in a specific tone, has trouble with social interactions or cues, and struggles to make friends. Maybe it’s the vaccination debate – if you’ve been around long enough, you’ve likely heard the social argument that “vaccination causes autism.” Or perhaps you’ve heard the term “autistic” thrown around as a derogatory slang term. Then again, some of us don’t even know what “autism” exactly is. Whatever it may be, the ever expanding subject of autism has made its way into modern day media through news, entertainment, stories, and even TV shows such as Netflix series Atypical, shaping the way that we define or view autistic individuals. Despite the stereotypes or television tropes you might have become familiar with, autism disorder is, quite literally, a spectrum – a complicated disorder that presents uniquely for each person, and one we are still far from understanding. Fortunately, advancements in research have allowed us to peer into the minds of these brilliant, fascinating individuals, and like most disorders, an understanding starts with studying things down at the cellular level. In this way, autism disorder is no different from the rest.
What is Autism?

The begging question still stands – what exactly is Autism Spectrum Disorder? Autism spectrum disorder, or ASD, as defined by the CDC, is “a developmental disability that can cause significant social, communication, and behavioral challenges.” This definition seems, frankly, quite vague. Typical symptoms include:
- Intellectual and verbal impairments, especially during development, failure to hit developmental milestones
- Repetitive actions and motions
- Problems with coordination and motor development
- Trouble interacting with, but having interest in others
- Prefer to be alone and avoid physical contact
- Trouble reacting to social cues
- Avoiding eye contact
- Does not understand sarcasm
- Lose skills they once had over time
- Hyperactivity
- ADHD
- Unusual reactions, temper tantrums
- Aggression and self injury
- Digestive or gastrointestinal disorders
- Potential seizures
For a full list of symptoms, be sure to visit the CDC’s ASD symptom page here.
But what’s the deal with the word “spectrum?” Because the severity of autism manifest themselves to varying degrees, the disorder is characterized by a spectrum. The stereotypical “gifted” child often depicted in media is an example of High Functioning Autism, characterized by someone who can function normally. For example, someone with Asperger’s Syndrome has a mild form of autism. They likely have deficits in social interaction and may either excel in school, or be stressed out by the social situation, but otherwise they can perform day-to-day functions. On the other end of the spectrum, there is Severe Autism. In this form of the disorder, those afflicted might struggle to perform day-to-day tasks such as getting dressed, eating, and even walking and sitting. The graphic below summarizes three notable markers on the autism spectrum.

Symptoms often manifest when a child is 2-3 years of age, and the disorder is often diagnosed around this time as well, though diagnosis is more common in males than females. Above all, what can explain the curiously diverse range of symptoms seen in a single disorder? Keep reading to find out!
[Autism spectrum disorder] is a developmental disability that can cause significant social, communication, and behavioral challenges
Where Does the Spectrum Arise – Why does ASD Happen?
As we learned, autism can present as various combinations of symptoms across the spectrum. Behind it all, though, what happens in the body that leads to such a vast array of symptoms? What dictates whether or not a child will be born “gifted?” Like many pathologies and disorders in modern medicine, it all traces back to the brain – that big, pink, wrinkly organ that dictates our every move, behavior, judgment, and thought. Down to the core, autism is largely a genetic disorder, meaning that the changes in the brain that predispose someone to autism are already there, even before birth (though that’s not to say that behavior of autistic children can’t be shaped by their social environment as well). Other factors, such as exposure to toxins and parental age can increase a child’s likelihood of developing autism as well. Despite some misconceptions, autism is not a result of poor parenting, and it is a legitimate brain disorder – thus the term “autistic” should not be used as a negative label or slang term.
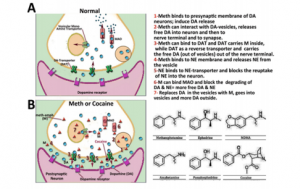
Fortunately, recent research has shed some light on the microscopic processes that lie behind the broad spectrum. Normally, when learning, neurons in the brain fire and result in one of two processes: long term potentiation (which results from high intensity firing and memory formation, such as reciting a word over and over to remember it) or long term depression (which results from low intensity firing and weakening of memory formation). To learn more about LTP , LTD, and synapses, be sure to visit my previous blog post, or the previous links. Both processes must be regulated to ensure a child’s brain develops properly, with just the right amount of neural connections, or synapses, in a process called pruning.

The best way to explore the spectrum is to find which genes are affected to begin with. Notably, these include:
- UBE3A: This gene is mutated or deleted in ASD. UBE3A normally codes for an enzyme that breaks down substances in cells. One of these substances is another protein, named ARC. The job of ARC is to reduce neuron excitation by pruning and weakening a synapse by removing AMPA receptors. When there’s too much ARC, too many of these receptors are removed, promoting LTD and decreasing synaptic strength.
- SHANK: This creatively named protein refers to a protein found in synapses. It is quite literally a scaffold that supports the placement of receptors. It’s safe to say that mutations in genes that code for SHANK proteins could result in defective scaffolds and poor or irregular placement of receptors in a synapse. This could lead to deficits in learning, memory, and development.
Depending on the severity of the mutation and the degree of biochemical damage done downstream, autism symptoms can manifest at various points along the spectrum. Because autism is so complicated, another easier way to understand the spectrum is by studying other disorders that share common mutations with the disorder:
- Angelman Syndrome: This genetic disorder often has a comorbidity of ASD and shares many common symptoms. Similar to ASD, it is marked by the loss of a gene called UBE3A.
- Tuberous Sclerosis: Also a genetic disorder, this syndrome is marked by mutations in genes called TSC1 and TSC2. Normally, these genes are tumor suppressors. Mutations in these genes might lead to the development of benign tumors, or too much growth or hyperconnectivity as seen in ASD.
- Fragile X: Yet another genetic disorder (see a trend here?). The gene at focus here is called FMR1, found on the X chromosome (as noted by the name, Fragile X). Mutation to this gene prevents the production of a protein called FMRP, which is important in proper brain development.

By connecting what we know about autism and similar disorders, we can get a small glimpse into the microscopic world that creates the spectrum and each unique case of autism. At the end of the day, some might find themselves asking, should we cure autism, if the advances of modern day technology and genetics allow us to? Throughout history, autism has been viewed as a gift, a blessing, and for some, a curse. For some, if a cure allows their child to eat, talk, sit, and even walk on their own, then a cure might be the blessing they need to improve their child’s quality of life. But then again, history has seen dozens of gifted individuals who have been, or are suspected to have been, on the spectrum. Among these are Hollywood director Tim Burton, actor Dan Aykroyd, and Scottish artist Susan Boyle. Records even suggest that the genius himself – Albert Einstein – might have shown symptoms characeristic of the spectrum! It’s no doubt that the contributions these people brought to the world have been gifts. But whether you view autism as a blessing or a curse, it all goes to affirm one true statement – at the end of the day, we are all, simply, unique.
For more information about autism, be sure to visit this page, by the Autism Speaks program.

 Autism spectrum disorder (ASD) is a debilitating development disorder. Frequent signs include impairments in social interactions and communication, and restricted, repetitive and stereotyped behaviors or interests. Autism is typically diagnosed in ages 2-3 but can sometimes be diagnosed later in life, especially in females. ASD is primarily a genetic disorder but can also be due to mutations. Some of these are:
Autism spectrum disorder (ASD) is a debilitating development disorder. Frequent signs include impairments in social interactions and communication, and restricted, repetitive and stereotyped behaviors or interests. Autism is typically diagnosed in ages 2-3 but can sometimes be diagnosed later in life, especially in females. ASD is primarily a genetic disorder but can also be due to mutations. Some of these are: and what is happening deep down. Autism is something that one is born with, but is not diagnosed until certain developmental bench marks are missed. Autism is diagnosed and then a spectrum is used to help define the severity. Some who are high functioning are considered to have Asperger’s. Autism is a complex disease and affects each person differently. However, even though they have a disease, they are still people living their life.
and what is happening deep down. Autism is something that one is born with, but is not diagnosed until certain developmental bench marks are missed. Autism is diagnosed and then a spectrum is used to help define the severity. Some who are high functioning are considered to have Asperger’s. Autism is a complex disease and affects each person differently. However, even though they have a disease, they are still people living their life.



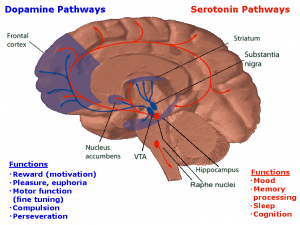
 factor causes more proteins to be produced than normal and affects the neural connections within the brain. Now, understanding slightly better what happens deep in the brain. So, is addiction within a person’s control?
factor causes more proteins to be produced than normal and affects the neural connections within the brain. Now, understanding slightly better what happens deep in the brain. So, is addiction within a person’s control?




 [5]
[5]