The neurochemistry course at Concordia College has been a pleasure to be a part of as it has solidified my interest in the mystery of the brain and led me to become a better scientist. As a neuroscience major, taking this class is a requirement for graduation. Although, I would recommend it to anyone willing to take on the challenge of understanding more about the fantastically complex interactions within the nervous system. I enjoyed discussing these brain pathways with a broad variety of individuals from an assortment of different backgrounds. This class allowed many different perspectives to be integrated into the ultimate interdisciplinary subject, neuroscience.
I have taken several classes involving the nervous system and brain, but none have given me the same sense of wonder or passion as provided from neurochemistry. It was a rewarding feeling to have finally accomplished all of the dirty work of understanding the basics of neuroscience and to apply it to a real-life problem. All too often do we get the sense that there is no point to anything we are learning in core curriculum classes. I spent countless hours studying brain regions and neural mechanisms of disease and got no sense of connection with the real world. But neurochemistry has made me realize what college is all about. This course allowed me to bridge the gap between what I know academically and what I know about humanity. There are a seemingly limitless number of diseases that can affect one’s brain and negatively impact their quality of life. Knowing more about just a handful of these diseases has provided me with a huge sense of fulfillment.
Another unique quality of this class was the emphasis on self-fulfillment rather than motivation through grades. Group projects in most classes involves splitting up an assignment, doing your own part, and never discussing or meeting with your group members. Although this can often result in good grades, no experiential learning occurs from it. Communication with others and self-efficacy are crucial skills to learn for our careers and the neurochemistry course has challenged us to pursue these goals. Neurochemistry is set up in a different way from most classes because it is more than just a grade on the line. We were not pushed to get a project done by its due date just to get a grade and be done with it. We worked on it because we had intrinsic motivation to create the best possible product. It gives me immense satisfaction to know that when I work hard on a difficult task, I can come out with something that has use in the real world. This goes for both group work and independent research. After taking this class, I am much more prepared to work on tasks independent from immediate reward.
The main project in this class was the community action project. This project involved a group of 8 people coming up with a plan to better the community. The issue we tried to solve was the fact that caregivers of trauma victims are not really educated on how the brain is involved with PTSD. We decided to reach out to a facility that cares for trauma victims in Fargo called Fraser. Our plan was to find a way to educate these workers about the neurobiology of the disease to help them achieve a better understanding of what is going on in the brains of these victims. Although the idea was simple, the difficult part of this task was to integrate just enough of what we learned in neurochemistry without overwhelming the workers with irrelevant knowledge. Overall, I think this project went well and the workers seemed pleased to have some education on this subject.
This community action project was another example of how neurochemistry has allowed me apply what I know in neuroscience to a real life problem. Before this project, my communication of science has mostly been through presentations to an audience that already has a solid understanding of what I was talking about. This time, I had to analyze the background of my audience and tailor my communication to a level that would provide the most benefit. This skill is important in any career as we all talk to people of various educational backgrounds and need to develop a sense of how to convey our thoughts effectively.
Something I really enjoyed in this class was the set schedule of events that happened each week. Mondays were set aside for initial discussion of the week’s paper and answering any questions about it. On Wednesdays we would discuss specific topics of the paper in more detail, and of Fridays a class discussion would be held focusing on the big picture implications of what we talked about earlier in the week. I enjoyed how we knew what to expect each class period and knew exactly what to prepare for. Also, these weekly discussions have allowed me to really get to know the entire class more than I have in any other course. I think it is very important to have a close relationship with colleagues and the neurochemistry course has exercised this skill. When a group of people know each other well, the final product they produce will often be better because each person finds out where they fit on the team.
I hope to use skills I learned in this class in the future as I believe many of them are useful in daily life. With the plethora of knowledge about neurochemistry I learned aside, the basic human skills to apply to the real world made this class worth it for me. It is true that I did learn a lot about brain diseases and ways to fix or improve them, but I think the biggest thing I can take away from this class is to never be satisfied with what I know. The weekly research we did on specific topics has made me realize that we will never be able to fully understand a topic and that there is always more research to do. As I pursue my career in the field of neuroscience research, I will keep in mind what I have learned from my capstone experience of neurochemistry at Concordia College.



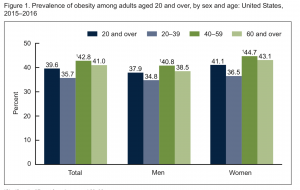
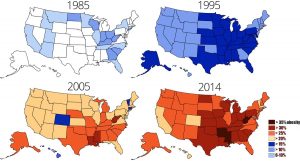
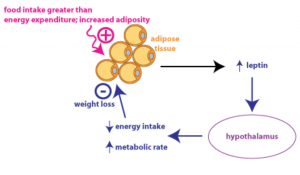
 Obesity is becoming more and more prevalent, as rates climb throughout both adult and youth populations. Around 40% of adults (over 20 years of age) are obese, as well as 20% of children. In the last 15 years alone these rates have shown a great increase. Obesity leads to the development of many serious health issues such as type 2 diabetes, hypertension, steatohepatitis, heart disease, stroke, cancer, depression, sleep apnea… the list goes on and on. To many people who are not obese, it seems as if there should be an easy fix to the obesity epidemic sweeping the nation: eat healthy and exercise. But what if I told you it is not as simple as that? What if I said that obesity can actually be classified as a neurological disorder? Because sometimes, there isn’t a simple answer to losing weight and keeping it off.
Obesity is becoming more and more prevalent, as rates climb throughout both adult and youth populations. Around 40% of adults (over 20 years of age) are obese, as well as 20% of children. In the last 15 years alone these rates have shown a great increase. Obesity leads to the development of many serious health issues such as type 2 diabetes, hypertension, steatohepatitis, heart disease, stroke, cancer, depression, sleep apnea… the list goes on and on. To many people who are not obese, it seems as if there should be an easy fix to the obesity epidemic sweeping the nation: eat healthy and exercise. But what if I told you it is not as simple as that? What if I said that obesity can actually be classified as a neurological disorder? Because sometimes, there isn’t a simple answer to losing weight and keeping it off.
 knowledge to succeed or understand the content in this class. Once we got into the rhythm of the class, I was pleasantly surprised that I was not as behind as I thought. Neurochemistry was a great class to have a capstone experience for many reasons.
knowledge to succeed or understand the content in this class. Once we got into the rhythm of the class, I was pleasantly surprised that I was not as behind as I thought. Neurochemistry was a great class to have a capstone experience for many reasons.