
Source: https://www.apa.org/helpcenter/recognizing-schizophrenia.aspx
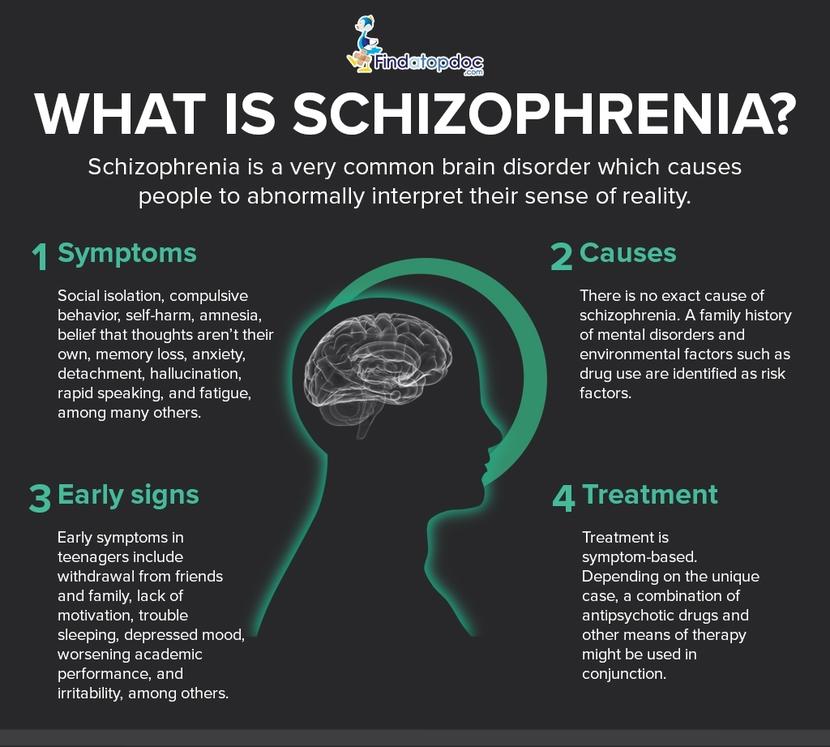
Recently in popular culture is has become a movement of acceptance and understanding when thinking about mental health. More often than not this just ends up including the more well know deviations from the norm and other disorders are left forgotten. One of the most misunderstood disorders is schizophrenia. Whether it be word of mouth, culturally, socially, or taught to us through the media there is a large misconception about what schizophrenia really is.
Dissociative Identity Disorder vs Schizophrenia
It is important to start here because this is the idea that many people have in their head when they think of schizophrenia. This tends to be one of the most common misconceptions, instead regarding schizophrenia as someone having multiple personalities. Multiple personalities, called Dissociative Identity Disorder (DID), is coupled in with three other types but of dissociative disorders but DID is characterized through the thought that one individual has multiple personalities. This stands in contrast to schizophrenia which often is disorganized speech, delusions, and hallucinations. An individual may also exhibit lesser known symptoms including abnormal behavior, unclear and confused thinking, and lack of motivation. Schizophrenia may also be presented with other mental illnesses as well, often observed in individuals with depression, anxiety, OCD, or substance abuse disorders. At its core, schizophrenia is a very different disorder from DID and it is critical to work toward understanding of both.

Figure 1: Here is a small table that briefly goes into more detail about the differences between DID and schizophrenia Source:http://www.differencebetween.net/science/health/difference-between-dissociative-identity-disorder-did-and-schizophrenia/
Hearing Voices
Although schizophrenia is often diagnosed through observing symptoms of delusions and hallucinations these behaviors are not exhibited 24/7. Along with the thought that schizophrenia is multiple personalities, many people also think that those with this disorder constantly hear other voices. Some people with schizophrenia do experience episodes that may include voices but about one fourths of individuals do not experience voices (auditory hallucinations). The diagnostic criteria of schizophrenia state that the patient must have at least one of the symptoms stated above, hallucinations and delusions, or disorganized speech for a period of one month.

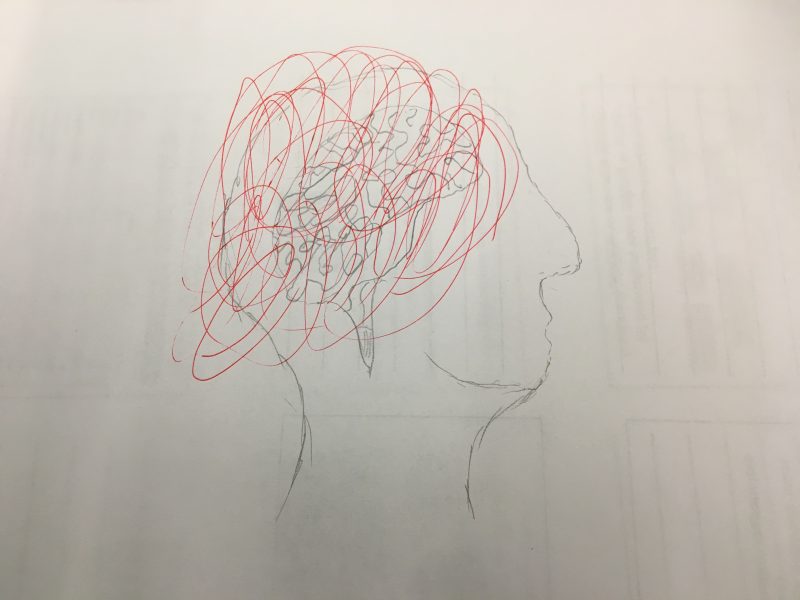
Figure 2: An artist’s illustration of what it is like living with her bipolar disorder. Although a difference disorder than schizophrenia, the overlying message is the same: sometimes there are voices but this is not something that is experienced by everybody.
Artist: Stumbling Mind — Katie
Source: https://stumblingmind.com/2017/02/06/doubting-myself-hearing-voices/
Other behaviors that are common with schizophrenia are diminished emotional responses, depersonalization, disturbed sleep pattern, and inappropriate responses. It is the case with some individuals that they may experience voices and hallucinations frequently but that may not be the same from case to case. Because of this lack of knowledge about schizophrenia and how it affects the people who have been diagnosed it causes a general sense of fear from the public, which tends to be exacerbated by media portrayal. This misunderstanding of the disorder is also linked to the thought that those who have schizophrenia tend to be dangerous.
People with Schizophrenia are Dangerous
Something that appears to be ingrained in human nature is to be afraid of things that we do not know. It is why people are afraid of the ocean and some fear the infinite depth of space. This is not only seen in phenomenons of nature but also throughout society. We do not understand those who are different from us in great degrees and so often the way that we view those types of people is tainted. As mentioned above, this includes the way that media shows us what is different influences our thoughts. It is far too common in movies and television shows that individuals who are behind the crime are affected by disorders such as schizophrenia. This adds to the stereotype that people with schizophrenia are violent and dangerous, which is not the case. Although schizophrenia may be unpredictable in actions most of the individuals who are affected live normal lives do not engage in violent activity. Even those who are receiving treatment for the disorder, according to one study, are no more dangerous than those who are not. It is essential to remember that the way that schizophrenia impacts someone is a spectrum and does not ring true for the next person.
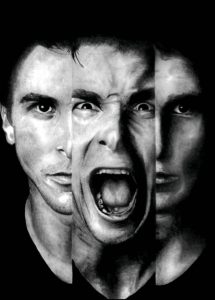
Figure 3: This is a compiled image of Patrick Bateman (played by Christian Bale) in the film American Psycho. Although Bateman’s mental health is not addressed, some speculate that he suffered from undiagnosed schizophrenia and adds to the stigma of those with schizophrenia being dangerous.
Source: https://www.chess.com/clubs/forum/view/playing-chess-benefit-schizophrenia-patients
It’s an Uncommon Disorder Caused by Bad Parenting
1 out every 100 people develop schizophrenia in the general population. There is a role of genetics as well in the disorder, the risk increasing to in regards to family members. Many people think that schizophrenia is uncommon, mostly because only the very sparse extreme cases are reported on and told to the public, but it is much more common than you may think. Although symptoms don’t begin to persist and become diagnosable until early to late twenties there is another myth that coupled with genetic factors, schizophrenia is due to bad parenting. This idea was proposed by a group of researchers in the 1950s with most of the blame falling on the mother. The claim today holds no ground but like what was observed with the falsifying of vaccine records, the public tends to hold on to things even though they might not be correct. High stress situations that take place at home may make the symptoms of schizophrenia but are not the cause of the disorder.
Figure 4: The myth that bad parenting causes mental illnesses such as schizophrenia has been discredited although some still refer to it.
Source: https://wundersameslernen.de/wieviel-ungehorsam-darf-s-denn-sein/
There are many rumors that cause the idea of what schizophrenia to be distorted but it is important to know the reality of the disorder. Understanding this group of our population allows for more education about the topic and ultimately to acceptance.
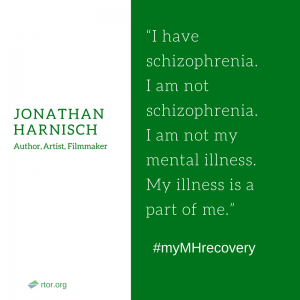
Figure 5: A quote from someone who lives with schizophrenia. It is his, and my, aim to inform everybody about schizophrenia to end the stigma attached.
Source: https://www.rtor.org/2016/08/23/quotes-on-schizophrenia/
Sources:
http://www.schizophrenia.ca/docs/Myths%20Half-truths%20and%20Common%20Misconceptions%20about%20Schizophrenia%20and%20Severe%20and%20Persistent%20Mental%20Illness%20(SPMI).pdf
https://www.webmd.com/schizophrenia/guide/schizophrenia-myths-and-facts#1
https://mentalillnesspolicy.org/medical/schizophrenia.html
https://www.verywellmind.com/dissociative-disorder-vs-schizophrenia-4160180
https://www.psycom.net/schizophrenia-dsm-5-definition/

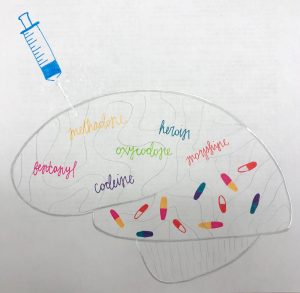



 Figure 3.
Figure 3. games, gambling and many other things of that nature. When one becomes addicted to drugs or any activity, the reward pathways in their brain are being altered which is when the addiction sets in.
games, gambling and many other things of that nature. When one becomes addicted to drugs or any activity, the reward pathways in their brain are being altered which is when the addiction sets in. longer sensitive to the everyday stimuli leading to the drug being the only stimulus to create this feeling of pleasure. The drug then eventually becomes less effective in creating this pleasure feeling and higher doses are needed to achieve the same feeling which can lead to overdose.
longer sensitive to the everyday stimuli leading to the drug being the only stimulus to create this feeling of pleasure. The drug then eventually becomes less effective in creating this pleasure feeling and higher doses are needed to achieve the same feeling which can lead to overdose.


 Another problem is that schizophrenia is usually not diagnosed until the late teens to early twenties making it impossible to catch the disease early. Many of schizophrenia’s positive symptoms, including delusions and hallucinations, can be attributed to normal childhood behavior like imaginary friends and make-believe games. Then in the teenage years, most parents and doctors correlate symptoms to hormone imbalances and puberty. There is also a lot of maturing and development that occurs during this time so many doctors don’t want to diagnose a patient prematurely.
Another problem is that schizophrenia is usually not diagnosed until the late teens to early twenties making it impossible to catch the disease early. Many of schizophrenia’s positive symptoms, including delusions and hallucinations, can be attributed to normal childhood behavior like imaginary friends and make-believe games. Then in the teenage years, most parents and doctors correlate symptoms to hormone imbalances and puberty. There is also a lot of maturing and development that occurs during this time so many doctors don’t want to diagnose a patient prematurely.
 Let’s be honest, the most information the general population receives regarding schizophrenia comes from movies, TV shows, and other forms of media. While these can be very entertaining, they do not often show the true story behind schizophrenia and how it can affect someone’s daily life. So let’s break it down: we will get a quick overview of what schizophrenia is before discovering what is causing schizophrenia in the brain and what it means to live with schizophrenia.
Let’s be honest, the most information the general population receives regarding schizophrenia comes from movies, TV shows, and other forms of media. While these can be very entertaining, they do not often show the true story behind schizophrenia and how it can affect someone’s daily life. So let’s break it down: we will get a quick overview of what schizophrenia is before discovering what is causing schizophrenia in the brain and what it means to live with schizophrenia.
 Until learning about the disease in depth, I previously believed that schizophrenia was interchangeable with multiple personalities disease. Rather, schizophrenia occurs when a person hears or sees things that are not truly real. They may appear to be disorganized and confused in their thoughts and conversations. Media and society has influences us to believe that schizophrenic people are violent and harmful to the outside world. However, that is a misconception. Very few schizophrenics are violent, and the ones who are, tend to have only random episodes of violence, not a constant state.
Until learning about the disease in depth, I previously believed that schizophrenia was interchangeable with multiple personalities disease. Rather, schizophrenia occurs when a person hears or sees things that are not truly real. They may appear to be disorganized and confused in their thoughts and conversations. Media and society has influences us to believe that schizophrenic people are violent and harmful to the outside world. However, that is a misconception. Very few schizophrenics are violent, and the ones who are, tend to have only random episodes of violence, not a constant state.