Featured image created by Julia Wolf and Microsoft CoPilot
The Science of PTSD
Not all stress is processed the same way by the brain. While many experiences are eventually filed away and lose their intensity, traumatic events can become deeply embedded, continuing to influence thoughts and emotions long after they occur. This starts with the body’s stress response. During a traumatic event, stress hormones like cortisol are released and travel to areas of the brain that handle emotion and memory, including the hippocampus and amygdala. These hormones don’t just signal that something important is happening, they actively shape how that experience is stored. Inside neurons, they activate receptors that set off signaling cascades, such as the ERK-MAPK pathway, which play a key role in forming long-term memories [1].
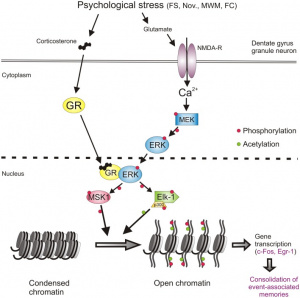
What’s happening at this stage goes beyond simple memory storage. Stress can influence how genes are turned on or off without altering the DNA sequence itself, a process known as epigenetics. This involves changes to histones, the proteins that DNA wraps around. When these proteins are modified, certain genes become easier to access, allowing the brain to strengthen connections between neurons involved in that memory. In other words, the experience becomes biologically “prioritized.” This system is normally beneficial because it helps us recognize and respond to danger in the future. However, in PTSD, this process becomes overactive. The brain may reinforce the memory too strongly, making it difficult to move past the event. Instead of fading, the memory is repeatedly reactivated, which can show up as flashbacks, nightmares, or persistent feelings of threat [1].
Anxiety further intensifies this cycle. Under typical conditions, the brain uses inhibitory signals, largely controlled by the neurotransmitter GABA, to keep stress responses in check. When anxiety is elevated, this braking system becomes less effective. As a result, stress-related activity in the brain increases, making traumatic memories more likely to be strongly encoded and easily triggered [1].
To learn more about the mechanisms involved in stress and PTSD, click here!
Comorbidities with PTSD
PTSD rarely occurs on its own. In fact, 80% of individuals with PTSD have at least one additional mental health condition, these comorbidities can significantly worsen outcomes, including functional impairments, reduced quality of life, and relationship problems [2].
Anxiety disorders are among the most common comorbid conditions. Disorders such as generalized anxiety disorder, panic disorder, and social anxiety frequently overlap with PTSD, largely because they share underlying features like hyperarousal, irritability, and difficulty concentrating. Generalized anxiety disorder, in particular, affects about 11.1-31.6% of individuals with pTSD and is strongly related to the hyperarousal symptom cluster. These shared symptoms reflect similar disruptions in the brain’s stress-response systems [3].

Substance use disorders are another major concern. Individuals with PTSD are two to four times more likely to develop substance use issues, and about 34.4% of those with PTSD also meet the criteria for at least one substance use disorder, most commonly alcohol use disorders. This is often explained by the self-medication hypothesis, which suggests that individuals use substances to cope with or numb distressing symptoms like intrusive memories or constant anxiety. However, this can create a cycle that worsens both conditions and leads to additional complications such as health problems and adhering to treatment [5].
Sleep disturbances are extremely common in PTSD and can further add to symptoms. Many individuals experience chronic insomnia or frequent nightmares, and some even develop a fear of sleep due to the possibility of reliving traumatic experiences. In veterans with PTSD, obstructive sleep apnea has been reported at rates of 43-75% [6], and about 90% of individuals experience insomnia symptoms, with around 40% meeting criteria for clinical insomnia. These disruptions not only worsen mental health but also interfere with physical recovery and overall functioning.
Beyond mental health, PTSD is also linked to a range of physical health conditions. Chronic activation of stress pathways can contribute to cardiovascular issues such as high blood pressure, as well as metabolic problems like type 2 diabetes and obesity. Individuals with PTSD also report higher rates of chronic pain conditions, including fibromyalgia, migraines, and arthritis, showing how deeply stress can affect the entire body [8].
Why This Matters
Understanding the science behind PTSD changes how we think about it. Rather than viewing it as simply a psychological issue, it becomes clear that PTSD is rooted in real, measurable biological processes involving brain signaling, gene expression, and long-term changes in how the brain functions. This perspective helps reduce stigma by showing that PTSD is not a sign of weakness, but the result of the brain’s attempt to adapt to overwhelming stress. It also shows why treatment can be complex, especially when multiple conditions occur together. Effective care often needs to address not just the traumatic memory itself, but also related issues like anxiety, depression, sleep disturbances, and physical health.
Most importantly, this research opens the door for better treatments. By targeting the underlying biological mechanisms, such as stress hormone systems, brain signaling pathways, and even epigenetic changes, scientists and clinicians can develop more precise and effective ways to help individuals recover.
References
[1] J. M. H. M. Reul, “Making Memories of Stressful Events: A Journey Along Epigenetic, Gene Transcription, and Signaling Pathways,” Frontiers in Psychiatry, vol. 5, 2014, doi: https://doi.org/10.3389/fpsyt.2014.00005.
[2] U.S. Department Of Veterans Affairs, “VA.gov | Veterans Affairs,” Va.gov, 2014. https://www.ptsd.va.gov/professional/treat/cooccurring/index.asp
[3] M. Price and K. van Stolk-Cooke, “Examination of the interrelations between the factors of PTSD, major depression, and generalized anxiety disorder in a heterogeneous trauma-exposed sample using DSM 5 criteria,” Journal of Affective Disorders, vol. 186, pp. 149–155, Nov. 2015, doi: https://doi.org/10.1016/j.jad.2015.06.012.
[4] J. Flory and R. Yehuda, “Comorbidity between post-traumatic stress disorder and major depressive disorder: alternative explanations and treatment considerations,” Treatment of Affective Dysfunction in Challenging Contexts, vol. 17, no. 2, pp. 141–150, Jun. 2015, doi: https://doi.org/10.31887/dcns.2015.17.2/jflory.
[5] J. L. McCauley, T. Killeen, D. F. Gros, K. T. Brady, and S. E. Back, “Posttraumatic Stress Disorder and Co-Occurring Substance Use Disorders: Advances in Assessment and Treatment,” Clinical Psychology: Science and Practice, vol. 19, no. 3, pp. 283–304, Sep. 2012, doi: https://doi.org/10.1111/cpsp.12006.
[6] P. Gehrman, “Sleep Problems in Veterans with PTSD – PTSD: National Center for PTSD,” Va.gov, 2014. https://www.ptsd.va.gov/professional/treat/cooccurring/sleep_problems_vets.asp
[7] G. G. Werner, D. Riemann, and T. Ehring, “Fear of sleep and trauma-induced insomnia: A review and conceptual model,” Sleep Medicine Reviews, vol. 55, p. 101383, Feb. 2021, doi: https://doi.org/10.1016/j.smrv.2020.101383.
[8] K. Jankowksi, “VA.gov | Veterans Affairs,” Va.gov, Mar. 02, 2023. https://www.ptsd.va.gov/professional/treat/cooccurring/ptsd_physical_health.asp
[9] Cleveland Clinic, “Post-Traumatic stress disorder (PTSD),” Cleveland Clinic, 2023. https://my.clevelandclinic.org/health/diseases/9545-post-traumatic-stress-disorder-ptsd