

As numerous studies have stated, concussions are mild traumatic injuries to the brain that result in swelling leading to further issues. So, being the sports crazed nation we are, how do we prevent brain injuries from occurring as well as taking the further precautions once they have happened? For starters, there have been a great deal of advancements from many equipment companies throughout sports that have been working to produce a helmet that both provides better protection as well as signaling when this protection was not quite enough to completely prevent someone from receiving a concussion.

From a hockey player’s prospective, I began skating before I was five years old and have gone from the Cooper helmets that were from the early nineties that offer about as much protection as if someone was to wear a 5-quart ice cream bucket on their head to wearing some of the newer brands like the recently bought out cascade helmets that were designed with concussion protection capabilities. Some companies are even beginning to work on placing sensors in helmets that detect the impacts taken during games and can signal when the impacts are reaching a severity that will require attention. How these work is they use a sensor that tracks both linear and rotational acceleration of the impacts and uses its signaling capabilities to transfer this data to a mobile app to keep record of the impacts taken during practices or games. The major piece being paid attention to is the rotational acceleration as that is the common factor in impacts that plays the greatest role in injuring the brain. During an impact that involves linear acceleration and no rotational acceleration, the brain is shifted in a front, back, or side-to-side fashion which is of course bad for the brain. At the same time these injuries have not been found to be as damaging the injuries that involve a bit of rotational acceleration as the impacts add another element to the brain injury. The rotational accelerations add a sheering force to the injury that causes not only a greater amount of damage but the twisting motion results in an overall faster, more forceful shifting of the brain resulting in more extensive injury.

Another attempt by companies to combat severe brain injury has been developed in the extreme sports market with a technology called MIPS or Multi-Directional Injury Protection System. MIPS has been an impressive advancement for brain protection as it works to protect from the extensive rotational acceleration injuries in athletes. This technology works by placing a layer that is fairly conforming to the top of the head as many helmets are designed to, but this thin layer is made from a material that has a very low friction coefficient allowing it to slide when a helmet receives an impact. By providing a sliding layer of protection, the brain has more defense against rotational acceleration as an impact occurs the outer shell may rotate as it hits the ground, but the MIPS layer will continue its normal trajectory thus preventing or lessening the added rotational element added to the impact.

These protective measures against concussions are not perfect but they are a good step in the right direction. It is important to continue the push for better technology to protect the heads of athletes especially children that have a great drive to be better athletes but do not understand the long-term consequences of brain injuries. Hopefully, in the future these advancements will keep getting more and more protective so parents don’t have to worry so much about the choice of whether it is a good idea to allow their child to participate in contact sports.
Fear, Anxiety, and the HPA Axis
To begin it must be made evident that Fear and Anxiety are in a sense necessary. We as humans thrive as a species because we have this innate response to fearful experiences. Our fears are responsible for activating the Hypothalamic-Pituitary-Axis (HPA) to elicit a stress response. This stress response allows our bodies to meet the needs of the stressful system to survive. The sympathetic response accounts for the adrenaline-like feeling we experience that can be described by elevated heartrate, respiratory rate, dilated pupils, and several other visceral responses. Most often, these responses are successful in helping us in acute fear eliciting instances.

The issue arises from the constant state of a fearful response which derives from anxiety. Anxiety is the state of worry that we might encounter our fears throughout our normal day of life. In some respects, this is a very helpful tool because it aids in keeping us alert when we are performing stressful tasks such as driving in the winter. The problem comes when our minds hold on to the anxious state during times that we should be in a parasympathetic state, or rest and digest as many might say. Many soldiers that come home from war experience this constant state of anxiety or in other diagnostic terms, post-traumatic stress disorder (PTSD).

PTSD is a common unfortunate burden soldiers bring home from wars that without proper coping or diagnosis can lead to severe issues. The problem in many cases of PTSD is the sudden sounds that elicit trained responses in these men and women causing them to act as they may have been trained to be prepared for combat. Furthermore, this issue leads them to further disorder such as chronic stress and depression.

Anxiety for most can be treated using several different methods, behavioral as well as pharmaceutical. Most commonly benzodiazepines are used as a treatment method for anxiety because it acts as an inhibitor of the system that activates sympathetic responses, leaving a more relaxed feeling instead of a stressful one.

Paired with anxiety that makes it such a harsh disorder is the fact that anxiety plays a huge role in memory formation. Being that fear is an innate trait we all have keeping us prepared for a stressful situation, we rely on memory to aid in recognizing dangerous situations. Long term potentiations play a dire role in memory formation due to the fact that they increase the ease of communication between our neuronal synapses especially in the hippocampus where we store our memories. The issue comes into play as we are not able to turn off these memories when we feel that they are causing great anxiety when a restful state is what should be called for. This is the ultimate unfortunate fact that those with great anxiety face as there is no cure for overactive memories especially those that cause us the greatest distress. Thankfully, behavioral therapy as well as mindfulness can help us cope with this burden as we attempt to carry on with normal day to day tasks.
Click This! Click This! Click This! and Learn About Addiction

Drug addiction is a hot topic of late, both with regards to scientific understanding and social action. The United States has been ramping up border protection in an effort to mitigate drug usage, and Portugal has legalized all drugs for recreational use in hopes of improving public health by de-stigmatizing drug addiction.
The question at the forefront of this issue is whether or not it is within our power to break away from our addictions.
Tackling this issue becomes difficult for several reasons. From a social standpoint, our society has been deeply influenced by Cartesianism ( https://en.wikipedia.org/wiki/Cartesianism ), and we think that our mind has the power to overcome every and all obstacles with sheer determination. The glorification of the mind over body mentality continues today with movies depicting soldiers and athletes overcoming their respective pain and achieving the goal they set out to achieve.
This is all fine and dandy, but it minimizes the power of the brain, and I believe it is the root of stigmatism in the U.S.
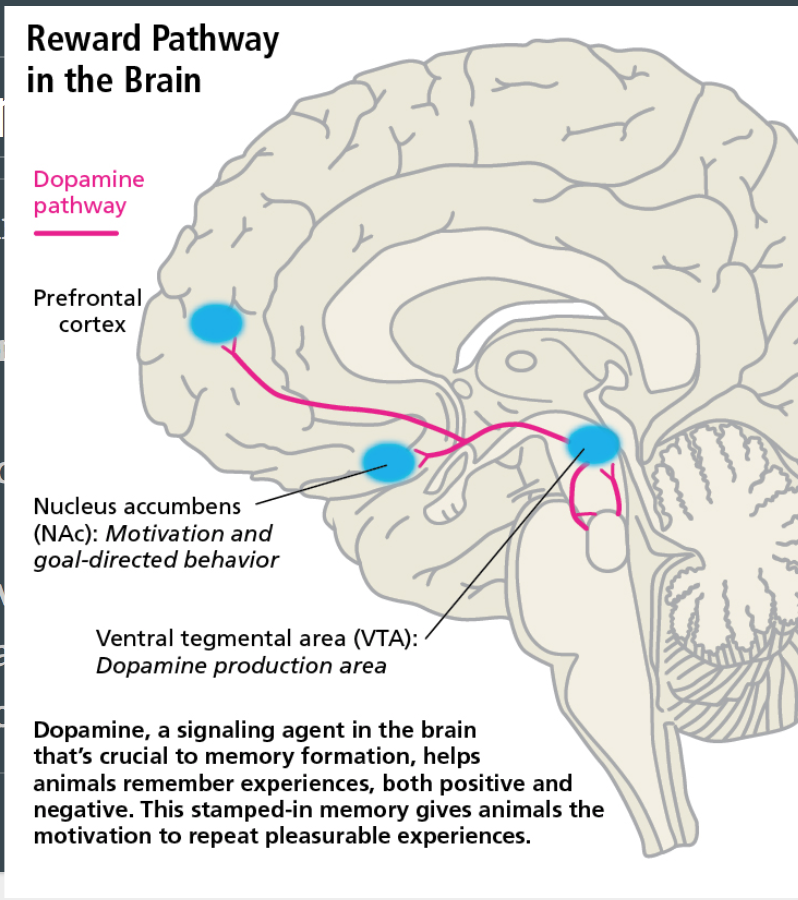
So what is happening in a person’s brain who’s struggling with addiction? For starters, addict’s “reward centers” in the brain are being overwhelmed. Our brains help us out by making us feel good whenever we do something that’s supposed to be good for ourselves. One example of this is eating some ice cream. Our brain processes the  signal from our mouth, and tells us “Ice cream good, eat more.” So we eat more because it feels good.This feeling good comes from a place in the brain called the Striatum (marked in green on the picture below). Our Striatum releases a neurotransmitter called dopamine, and we receive a feeling of pleasure.
signal from our mouth, and tells us “Ice cream good, eat more.” So we eat more because it feels good.This feeling good comes from a place in the brain called the Striatum (marked in green on the picture below). Our Striatum releases a neurotransmitter called dopamine, and we receive a feeling of pleasure.
Drugs:
So where do drugs fit into all of this? Particularly addictive drugs like methamphetamine and heroin hijack your Striatum. These drugs cause a huge amount of dopamine to be dumped into your brain and cause a feeling of intense pleasure and euphoria. Herein lies the problem with drug addiction. The Striatum’s job is to promote continued action by making us feel good. When we stimulate that region of our brain with an action, such as taking some prescription pills or illegal substances, our brain becomes hardwired to wanting to repeat that action. The dial gets turned up to 11 when we do this with addictive drugs because of the amount of dopamine released. Several proteins and cellular pathways become activated in our brain to rewire it. Some of the proteins such as protein kinase A and C serve to cause cellular restructure and proliferation.
When we take all that’s happening to our brains into account, we see that drug addiction becomes less and less of a choice and more of necessity. Our brains become trained to want drugs more than things like life-sustaining food. It seems confusing that our brains would rather have drugs and die instead of being healthy. But that’s because living healthy doesn’t always activate our striatum. Simply put, our brain gets turned against us when addictive drugs are put into the equation. We become erratic and irrational.
Regardless of your stance on drug addiction, please let anyone you know struggling with addiction that there are people out there who are willing to help them without any judgement. The hotline for drug abuse is 1-877-978-2486, and you can find there website here http://drugabuse.com
Recapping the Capstone

Neurochemistry sounds kind of scary, doesn’t it? Well let me tell you that it was a great class. The structure and organization of the class created a great environment for all the students to have interesting dialogues. We learned about a neurological disease every week from a scientific literature standpoint. By doing this we discussed the paper in full, researched new topics relating to the disease, and had open dialogue to discuss the disease. This has been one of my favorite classes at Concordia College and any upcoming senior should definitely consider taking it. Mental health diseases affect so many people around the world and so many of our friend and family either know someone affected or are affected. By taking this class you can further your knowledge on these topics and develop an understanding and compassion for people that suffer from these diseases.
We also were required to do a community action project where we had the opportunity to spread awareness of a disease of choice. This was a great project that I had a lot of fun taking my time and effort to actually do something concerning a disease. I will miss the weekly couch dialogues every Friday and listening to everyone’s opinions. Thank you Dr. Mach for a wonderful experience!
It Is Time to Think Differently
What do you think when you hear the word “addiction”? Do you think that it’s a choice? Do you stigmatize people who are claimed to suffer from the word “addiction”? What if I told you that addiction is a disease? What would you say? Well….. I’m here to argue that addiction is a biological disease.
First lets define what addiction is.
The International Statistical Classifications of diseases and Related Health Problems (ICD-10) defines addiction, characterized as uncontrollable and unpleasant mood states leading to compulsive drug seeking behaviors and taking the drug despite negative consequences. The ICD-10 is a criterion for diagnosing diseases that was created by physicians, psychiatrists and psychologists. A disease is defined by “a disorder of structure or function in a human, animal, or plant, especially one that produces specific signs or symptoms or that affects a specific location and is not simply a direct result of physical injury.” What I hope to do now is explain why addiction fits into the general definition of a disease.
A review article in the Frontiers of Neuroanatomy journal explains how addiction affects the striatum, (which is an area in your brain) as well as the signal transduction in your brain that is responsible for not only cell activity but also for how you think, feel, and behave. Addictive substances bind to receptors in your brain which then releases neurotransmitters such as glutamate and dopamine and carry out their effects in this way. The striatum is an important area when researching and discussing addiction as this area of the brain contains the Nucleus Accumbens (NAc) and the Ventral Tegumental Area (VTA), which are involved in the mesolimbic reward system.
The brain reward system is responsible for making you feel good or a reward from a certain stimulus. Drugs of abuse target this natural biological mechanism and hijack it to manipulate the individual to form stronger memories that are related to drug seeking behavior.
.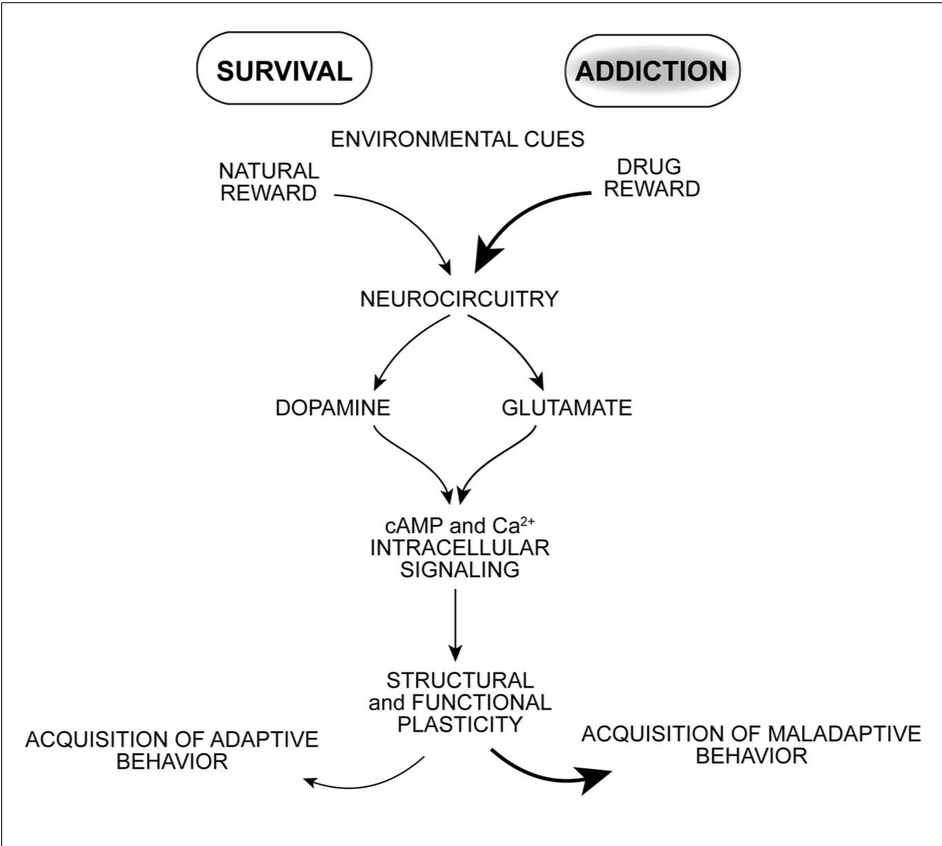
Drugs can induce proteins to be created to change and strengthen neuronal connections within the brain that favor maladaptive behavior. Chronic Drug Abuse is characterized with the built up of pharmacological tolerance, dependence and sensitization. Tolerance is characterized as needing more of the drug to experience the same “reward”. Dependence is characterized as experiencing withdrawal symptoms if the intake of the drug stops. Sensitization is the experience of the individual to crave the drug. The reason why these aspects occur is because receptors in your brain change their composition in number because there is so much neurotransmitter readily available that your body does not need as many receptors. So once drug intake ceases there is not enough neurotransmission occurring because there is a decreased amount of receptors and this is when the individual experiences withdrawal symptoms. Withdrawal symptoms vary by drug specificity but some examples are sweating, headaches, tremors, nausea, irritability, etc. People can overcome addiction by completely abstaining from the substance but are at high risk for relapse for many years after.
So, I think I have established a specific structure in the human body that is dysfunctioning and as a result the individual experiences withdrawal symptoms and compulsive drug seeking behavior that is unavoidable. Doesn’t this fit into the general definition of a disease? It’s weird to think that your brain is a part of your biological body. I’m not sure why people try to separate it. But anyways, the causes and risk factors for addiction exist in a broad spectrum. It could be due to social peer pressure, genetic predisposition, prescription drugs, dealing with a life hindrance, or taking drugs to escape other symptoms from comorbid mental illnesses.

Addiction affects around 20 million Americans and around 1 and 10 people suffer from the disease. Around 100 people die everyday from drug overdose in the United States and in 2015 drug overdose claimed the lives of over 50,000 people. Addiction doesn’t kill just by overdose deaths either; other factors such as accidents and suicides are a huge problem with the prognosis of addiction. It is time to change the way we view addiction as a society so that we can create progressive changes and stop these senseless deaths and crimes.
Pathways of Schizophrenia
I am a uniquely situated person. I am a biochemistry major with a sociology minor. At this point in time it puts me in both an introductory sociology class and my upper level chemistry course about the chemistry of the brain. This put me in an interesting position while discussing mental illness in sociology. The idea that mental health is dependent on how you were raised and what experiences you have is a problematic idea. Now that is not to say that how you were raised and your experiences do not shape mental illness but to say that you have your mental illness because of how you were raised is not okay. Take for example schizophrenia.
Schizophrenia is a mental disorder where individuals experience hallucinations or paranoia. These hallucinations can be seeing  things that are not there, hearing things, and smelling things that are not there. Paranoia can be thinking that someone is trying to kill you or delusions of grandeur. One of the good examples of schizophrenia in the media is the movie “A Beautiful Mind”. The movie is about the journey of a very famous mathematician John Forbes Nash Jr. and how he experienced schizophrenia. One of the most saddening moments of the movie is when he is walking through the crowded campus yelling at his hallucinations. One of the greatest struggles with being diagnosed with schizophrenia is that patients then have to understand and accept that they way they see the world is not real.
things that are not there, hearing things, and smelling things that are not there. Paranoia can be thinking that someone is trying to kill you or delusions of grandeur. One of the good examples of schizophrenia in the media is the movie “A Beautiful Mind”. The movie is about the journey of a very famous mathematician John Forbes Nash Jr. and how he experienced schizophrenia. One of the most saddening moments of the movie is when he is walking through the crowded campus yelling at his hallucinations. One of the greatest struggles with being diagnosed with schizophrenia is that patients then have to understand and accept that they way they see the world is not real.
The reality of schizophrenia is it is not very common. According to the National Institute of Mental Health only approximately 1.1% of people in the United States have the disease. However that can range from mild to very severe cases. This can be a very hard thing for patients and their families to deal with. That is one of the reasons that looking at schizophrenia as if it is caused by how a person was raised is really problematic. Not only do individuals have to deal with the disease and all that is involved but then it is also their fault that they have it in the first place.
THIS IS NOT TRUE.
Schizophrenia is caused by chemistry in the brain. In particular neuroscience suggest that it is due to imbalances in the Wnt pathway. Pathways are what we call the rout that signals take from the outside of the cell to other parts of the cell. It is similar to a game of telephone. A receptor on the outside of the cell gets a signal it then tells a signaling molecule who tells another signaling molecule and the signal is sent to where it needs to go, in this case the nucleus. In the Wnt pathway, Wnt is the receptor that starts this molecular game of telephone. Now it should be said that molecules are specifically better at telephone than most human beings so there are more options for what the end of the telephone game will be. In the one pathway signals can be sent to the nucleus where genes are expressed or it can directly effect other parts of the cell. Also molecules are good at stopping pathways after the signal is sent to there is not too much information happening at once.
One of the biggest players in the Wnt pathway is GSK. GSK helps to send the molecule beta-catenin in to the nucleus to express genes that are necessary for the cell. What is proposed in schizophrenia is that GSK does this job to well and there is too much beta-catenin entering the nucleus. The extra beta-catenin causes over expression of memory genes and may cause the formation of signals that are not really there.
Schizophrenia is still not fully known and so more research should be done to understand how this pathway can be regulated but one thing is certain. It is not an individuals fault if they have schizophrenia and the best thing we can do for them is to help them understand that and make it easier to seek out treatment.
Reflections on My Experience at Concordia College

Liberal arts education provides a wide-breadth of knowledge for students to deal with the ever changing and complex problems facing our world today. This is the foundation that Concordia’s educational mission statement is based upon.
“The purpose of Concordia College is to influence the affairs of the world by sending into society thoughtful and informed men and women dedicated to the Christian life.”
As students at Concordia, we complete a core curriculum that provides educational experience in areas outside of our primary focus. This includes language, science, religion, arts, and history.
If you happen to ask any student about what this means for them, you will most likely have the term “BREW’ing” yelled at you. This term is frequently used on campus and stands for Becoming Responsibly Engaged in the World.
It is the idea that behind learning connections between diverse areas of study and how that can be used to make positive impacts locally and globally.
Personally, at the begging of my education I did not fully grasp what BREW really means. My ‘aha-moment’ came during a religion class where I made connections between the importance of understanding the issues facing societies across the world through different perspectives. For example, how religion can act as a source of empowerment for marginalized groups that can bridge gaps in literacy, healthcare, and more.
A recent psychology course I took also brought my attention to an issue of the career path that I am currently on. This is the gender disparity that exists in science, technology, engineering, and math (STEM). A metaphorical leaky pipeline exists that describes the loss of women at all stages along the STEM pipeline.
I was inspired to BREW and do something about it. I participated in an outreach program that encourages young women onto the STEM pathway. The experience inspired me to continue efforts after my time at Concordia and into my own science career.
The neurochemistry course I took this semester was the culmination of my global liberal arts education. Through this class, we learned how neurometabolic pathways are impacted by environmental and biological factors associated with disease pathology. Topics included stress, obesity, neurodegenerative disorders, and more. We also had the opportunity to engaged the community regarding these issues. Communication of current science with the public is important for improving outcomes of these diseases. My group focused on raising awareness for the critical need for Amyotrophic Lateral Sclerosis (ALS) research and support.
If you have been on social media recently, you may be aware of the current fight for science regarding issues facing the scientific community. A major disconnect exists between the scientific community and public. Part of the blame falls to scientists that for too long have neglected this relationship. Members of the scientific community need to more effectively communicate to separate facts from misconceptions. This will demonstrate the importance of science with improving many aspects of society.
BREW’ing during my time at Concordia has helped me identify, and creatively help solve issues such as this. I plan on using the skills gained during my time here to do my part as a engaged citizen. As a young hopeful scientist, I have a passion for issues in regarding STEM. I now have the tools and drive to make lifelong positive impacts and I have my liberal arts education to thank for that.

The Cracked Stone

I know Concordia is trying really, really hard to meet its “Five Goals of Liberal Learning”. Before I begin talking about these goals, it might be important to state them.
- Instill a love for learning
- Develop foundational skills and transferable intellectual capacities
- Develop an understanding of disciplinary, interdisciplinary and intercultural perspectives and their connections
- Cultivate an examined cultural, ethical, physical and spiritual self-understanding
- Encourage responsible participation in the world

And I am not going to lie, the liberal arts education I have received here has certainly met these goals. But has my “capstone experience”?
There are a few things to recognize about the capstone experience before we examine it further. First, it is a class that graduating seniors are required to take. Second, these classes are given the “capstone” listing with the understanding that they emphasize learning in a broader sense than typical classes (i.e. not from textbooks). Indeed, the Concordia College website defines the capstone as follows:
The Capstone Course sequence of the core curriculum focuses on student achievement of the Goals for Liberal Learning, and emphasizes writing intensity and experiential learning. These courses have students reflect on the Goals for Liberal Learning and thus reinforce the connection between liberal learning and various academic disciplines. This part of the new curriculum was implemented in the 2010-2011 academic year. Faculty development will be devoted to managing capstone course development in each academic division.

I worry that Concordia has backed itself into a corner with this definition. How is it that a student can gain a “love of learning” when they are forced to take a class they may not be interested in? Of course, this is the precisely the reason why a large variety of capstone courses are offered: so that a student may find one interesting enough to take. But I was not allowed that choice. The ACS chemistry major (biochemistry concentration) lists neurochemistry as a required course. When I saw that listing, in and of itself, the class was changed from a “liberal learning” course to “just another chemistry course for my major”. It loses all other qualities, simply from my recognition that it was no longer my choice.
Indeed, I love(d) chemistry, and the course was also quite enjoyable from that standpoint. But it was not a “capstone” experience (for me). I wish I could say otherwise, but I would be lying. The writing assignments still felt like assignments, and the tests still felt like tests. And honestly, I cannot complain about the class itself, as I learned much. But to insist that the class behaved in capstone sense (for me) would be fallacious.
Regarding Concordia’s “Five Goals for Liberal Learning”, I had already met them, quite likely during my second year, if memory serves. And thus, as I see it, there is no benefit to the “capstone” experience being labeled as such. If Concordia is truly the strong liberal arts institution I regard it to be, the existence of such an experience is moot. Might I offer a solution that can make both the students and the administration happy?

Students are here to learn, but they do not want to learn everything that is asked of them. Yes, this is hypocritical, but for all intents and purposes this is the truth. Ask any student if they enjoy their homework, and the response will be “no”. And so clearly it follows from this that to “instill a love of learning”, Concordia must ensure that students can pursue their own paths of learning in a subject, however niche or specific that subject may be. And what could the students gain because of this (instead of a grade on a transcript like the capstone course gives)? The students could create whatever they feel fit to create. We already have a Celebration of Student Scholarship each spring. Could it not just be an extra requirement to make seniors showcase their projects then?
What I am proposing, in its most simple sense, is this:
- Set up a 1-or-0 credit class that is called the “capstone”.
- Let a student pick a faculty member to work an independent study (one-on-one) with. They can meet once per week.
- The student must produce something tangible (g. a book, published journal article, work of visual art, composed music, theatre event) to be showcased at the end of the year
- The faculty member gives the student an appropriate grade based on perceived work ethic. (This could even just work as a pass/fail.)
The reason this should work well, is that by senior year, most students have figured out where their passions lie, and if they have not, a single “capstone” class isn’t going to be a “massive epiphany” to them, but conversations with a respected professor might. Even further, this allows each student to leave the institution with something that they can look back at and marvel, saying “I did that”. Administrators would be happy too, seeing a drastic increase in student research and publication (i.e. something they can brag about when trying to convince prospective students to attend).

Did my neurochemistry course mimic anything remotely like this? Sadly, no. Simply put, I learned about neurochemistry. What a “life-changing”, “mind-bending” experience that “prepared me to conquer the problems of the real world” and “instilled a love of learning” in me. Indeed, I almost felt as though sometimes it did the opposite. This semester I had a mathematical breakthrough that will likely change the course of modern mathematical research, and instead of being able to devote my time where it was most efficient, I was writing blogs about neurochemistry that would never be read by more than a handful of people.
Perhaps I have become a cynic, but perhaps there is something inherently flawed about the capstone experience. I am not arguing against neurochemistry as a class, but rather the “capstone” subdiscipline with which it was assigned. I know this blog was supposed to explain how this class met the goals, but my morals got the best of me and I had to tell the truth. And please, don’t take my opinion as the tried-and-true fact; it is likely I could be the exception rather than the rule. If the opinion of the majority is in support of the capstone, then it is likely the best option.
With that said, I believe there is going to be a change in the capstone experience very soon. It is being replaced by PEAK (I don’t know if it is meant to be all capitalized, as I have only heard of it by word-of-mouth). And with any luck, this will let future students avoid some of the cynicism that I have felt my final semester of college.
(Don’t worry about me though, I am truly quite content with life right now. This was just my opinion regarding a very small matter, that in the end will not make much of a difference.)
Autism Is More Than Genes
Diseases like type 1 diabetes and sickle-cell anemia happen through a defect in a single gene. Sometimes all it takes is one wrong letter in the genetic code to create a life-threatening disease. If only autism were so easy to understand and treat.
Unlike diabetes, autism cannot be explained simply by proteins or genes. Diabetes has several obvious symptoms (frequent urination, excessive thirst, and exhaustion), it has one absent protein, and it has one mutated gene. Autism is in another world of complexity on several levels.
First of all, autism itself is a slippery disease to diagnose. Different people have different classic symptoms at different severities. Sometimes autism is mistaken for ADHD or language difficulties, and vice versa. There is no biological test for autism like there is for diabetes.
Second, in autism, there is no single gene that explains the symptoms. When we sequence the genomes of patients with a disease, sometimes we find one gene that is defective in all patients. Diabetes is a great example of this. We knew for decades that diabetics were incapable of making insulin, but only genetic sequencing could show that the cause was actually quite simple: the instructions for the insulin protein were mutated. Only about fifteen percent of autism cases across the spectrum can be pointed directly to genes. Multiple genes are involved, and some combinations of mutations seem to be worse than others. These relationships are too complex for even the smartest scientists to understand.
Twins can tell us a lot about the importance of genes in a disease. When one twin has autism, what are chances their identical twin also has autism? There is a 77% chance for males and 50% for females. Why don’t these other twins all have autism as well? Something must explain the difference.
The missing factor in autism is the environment. A similar relationship happens in cancer. Cancer runs in families, so part of a person’s risk for cancer comes from harmful genes. The other part of the risk comes from lifestyle. A person with resilient genes may avoid cancer by living cleanly, but could still get lung cancer if they smoke three pack a day. Likewise, someone with cancer genes can breathe only air their entire life and still develop cancer.
Viral infection is one non-genetic thing that can add to autism risk. A viral infection at a critical point in development before birth can alter the immune system of both mother and child, and eventually alter the fetus’s brain. Vaccines are probably a vital part of autism prevention.
A mother’s mental stress can explain some cases of autism. This is true before birth and during birth. For example, autism tends to increase after large groups of pregnant women experience disastrous events such as violent storms. The trauma causes the release of stress hormones, which activate the mother’s immune system and can harm the baby’s developing brain. Stress during birth can increase complications like low oxygen supply to the baby, which is of course harmful to the brain. The old wive’s tale that traumatizing a pregnant woman will harm the baby probably has a grain of truth.
Not only is autism a disorder of multiple genes, but lifestyle and environment of the mother are involved, too. Many connected factors come together to produce many complicated effects. It may turn out that the thing most affected in autism is the way our neurons are connected and knit together to send signals across the brain. One molecule injected in someone’s veins probably can’t fix that. However, by the time we understand autism enough to cure it, we will probably have understood it enough to lessen the burden we put on the autistic and maybe even appreciate what only they can add to our lives.
Capping the Stone – The Culmination of My Concordia Experience
If any one of you decides to attend Concordia be prepared to hear a lot about BREWing. However, unfortunately this BREWing is not of the alcoholic variety (generally). So if you were getting excited there for a second I apologize. So for the few that are still reading this article and want to know more about Concordia’s academic goals, BREW is an acronym for Becoming Responsibly Engaged in the World. And I can understand if this definition sounds like nothing more than pretentious academia gobbely-goop that people use as ammo against liberal arts colleges. However, the concept of BREW has intentionally bled into every one of my classes at Concordia from the driest of math lessons (no offense math) to the lofty existential discussions in religion that have made me question my entire purpose.
The concept of BREW was at its most importance in my Neurochemistry capstone course as the function of a capstone course is to take all that you’ve learned with you liberal arts education and put it together to create something meaningful (a.k.a. BREWing). And I will say with utmost sincerity I truly felt that happened in Neurochemistry. We covered a variety of difficult topics like obesity, Alzheimer’s, ALS, mental illness, and addiction in a very nuanced way. Of course the primary aspect of these diseases that we covered were related to neuroscience. However, the most important thing that was stressed in this course was that science doesn’t exist in a vacuum. In real life scientists don’t just sit in dark rooms spouting off random scientific jargon at each other and either agreeing or disagreeing with each others’ findings.
What makes science important and special is when findings can be conveyed accurately to the public as well as being able to make a real world impact. Furthermore, science is directly affected by larger forces such as society, culture, economics, business, and politics. And these topics were brought up many times. Questions like how can we relate to people that vaccines don’t cause autism or is there even a scientific way to treat the obesity epidemic were brought up. I know that as a freshmen going into college I wouldn’t have been able to even think up these sort of question let alone look at them in a multifaceted way. How we can impact and respond to a world where it seems like everything is becoming more and more complicated is important. What’s even more important is being engaged in this crazy world in a responsible and informed manner – especially since there seems to be an even bigger blurring of information despite so much of it being readily available. And now on the cusp of graduation, I feel like I’ve reached a point where I can.