In the United States there has been much discussion about drug use over the past several decades. Of course this all started with the War on Drugs which was first mentioned by President Richard Nixon in 1971. However, the United States has been combating drugs since the Harrison Narcotics Act of 1914. This ultimately led up to the formation of the Bureau of Narcotics in 1930. Since then there has been many new drug laws being put on the books. Ultimately the drug scare arose in the Comprehensive Drug Abuse Prevention and Control Act of 1970. This led to the first mandatory minimums and some people would argue to the rapid rise of incarceration in the United States. That is a topic for another post.

In the modern day and age it is estimated in 2013 that approximately 24.6 million Americans (9.4% of the population) had used drugs in the past month, according to the National Institute on Drug Abuse. This was an increase from the 8.3% of the population in 2002. However, one important thing to note is that the National Institute on Drug Abuse estimates that the number of people that are dependent on drugs is decreasing. Even if this is the case it is still important to understand what is occurring in the brain and how someone can get help if they need it.

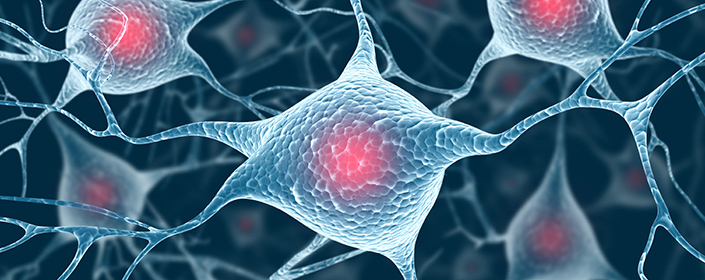
First it is probably best to explain what occurs in the normal brain. In the normal brain there are dopamine receptors and glutamate receptors located on medium spiny neurons. Medium spiny neurons are GABAergic inhibitory neurons that comprise about 95% of all neurons in the striatum/basal ganglia. The receptors discussed above bind dopamine and glutamate, respectively. These molecules when released bind to their respective receptor and cause downstream signaling that can lead to memory formation, motivated behavior, reward learning consolidation, and synaptic remodeling. It is important to remember that this is a natural process and occurs every day.

Now when drugs of abuse enter the body they alter dopamine and glutamate neurotransmission. The primary receptor targeted is the dopamine receptor because of its primary role in the reward system and their interaction with glutamate receptors to signal reward learning. Underlying regulatory mechanisms of these receptors become altered and ultimately lead to functional and structural neuroplasticity. Basically, what I am saying is that drugs can alter the behavior and function of the receptors to promote the addictive state. This ultimately can lead to hyper-synaptic remodeling, overwhelming reward learning, and uncontrollable drug-seeking and drug-taking. This leads to a never ending cycle that can cause an addict to have uncontrollable urges to obtain and take drugs. Inevitably this may lead to such a reliance on the drug that the addict may ultimately die to the body’s dependence on it. One important thing to note is that since the drug causes structural and functional alterations to the brain, withdrawals can be severe and going “cold turkey” may actually do more harm than good.
If you know anyone that is addicted please reach out to help them to prevent these scenarios. Get them help and be there for them as support to make it through the process.
![]()