What you might have missed amid the election results last Tuesday were the number of new marijuana laws that passed. Four states, California, Maine, Nevada, and Massachusetts, passed laws for recreational use and now join four other states plus the District of Columbia with similar laws. Additionally, North Dakota, Florida, and Arkansas each passed medical marijuana laws bringing the total to 28 states and the District of Columbia with similar laws.
And while I’m happy the law I voted for in North Dakota passed, I was honestly surprised that my ultra conservative state passed the law so easily (64% in favor). But perhaps the resounding decision in North Dakota represents a broader change in opinion across the United States regarding marijuana, despite it still being classified as a Schedule 1 drug by the United States. My thinking is that North Dakota’s decision represents a willingness to view marijuana as more than an illicit drug and consider its medicinal value. However, before you jump on or off the cannabis bandwagon, don’t you think you should how it works in the brain first?
You’ve probably heard of THC before and you might know that it’s an active ingredient in marijuana. The full name for THC is delta-9-tetrahydrocannabinol and has the chemical structure shown below. THC is classified as a cannabinoid, but what you might not know is that we have cannabinoids in our body that are produced naturally. These most common endocannabinoids are anandamide (AEA) and 2-arachidonoylglycerol (2-AG). What might not be entirely evident is that all three of these molecules share a common receptor called a brain cannabinoid receptor (CB1).

The CB1 receptor is a G-protein coupled receptor that is highly expressed in the hippocampus, cerebral cortex, cerebellum, and basal ganglia. The CB1 receptor is essential to marijuana’s effects because it binds THC and our own endocannabinoids, leading to the downstream physiological effects of marijuana. An interesting point to understand is that the CB1 receptors are concentrated on the pre-synaptic neuron whereas our endocannabinoids are released from the post-synaptic neuron. To understand the effects of THC, however, we must first understand our own endogenous pathway in the picture drawn below.
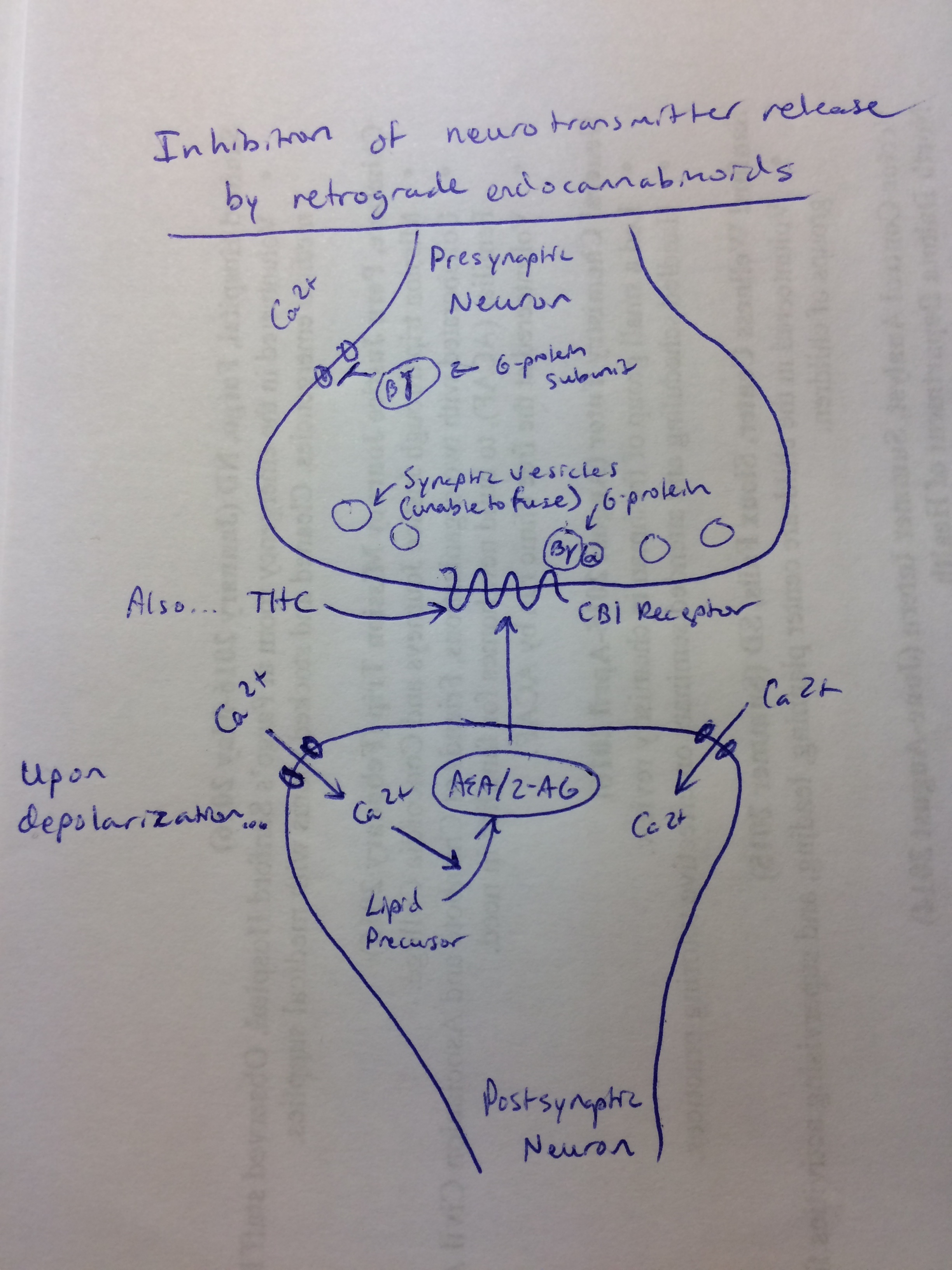
Depolarization (increased cell voltage) of the post-synaptic neuron leads to the opening of voltage-gated calcium channels. When calcium rushes into the post-synaptic neuron, it activates enzymes that synthesize our endocannabinoids (2-AG and AEA) from lipid precursors. The newly formed endocannabinoids then exit the post-synaptic neuron and diffuse to the pre-synaptic neuron where they bind the CB1 receptors. This seemingly backwards path is known as retrograde signaling.
When THC or one of our endogenous cannabinoids binds CB1 on the pre-synaptic neuron, it ultimately suppresses neurotransmitter release by decreasing the ability of synaptic vesicles to release their contents. This is a result of activation of CB1, which inhibits pre-synaptic calcium entry through direct inhibition of calcium channels by the beta and gamma subunit of the G-protein coupled to the CB1 receptor.
We know generally that cannabinoid signaling through CB1 leads to inhibition of neurotransmitter release, but what you have to realize is that not all neurotransmitters lead to more activity. In fact, both inhibitory and excitatory pre-synaptic neurons, releasing GABA and glutamate respectively, can be inhibited by cannabinoid signaling. I won’t specifically discuss how these opposite effects can be modulated leading to increased appetite, reduced pain, and reduced memory formation, but the general signaling always comes down to CB1 activation and inhibition of neurotransmitter release.
So when someone smokes marijuana, their entire body is flooded with the exogenous cannabinoid THC, which subsequently binds to CB1 receptors. This reduces the ability of our endogenous cannabinoids to bind the receptors themselves and regulate the cannabinoid response, which in turn leads to the effects we are familiar with after marijuana use.
How Weed Works