“Autism is neurodevelopmental disorder characterized by impairments in communication, social behavior, and repetitive behaviors” https://moodle.cord.edu/pluginfile.php/468408/mod_resource/content/1/autism%20and%20environ.pdf
Causes of Autism:


- genetic mutations
- Environmental factors
Genetic mutations: in genes responsible for encoding proteins involved in the signal transduction form the synapse to the nucleus signaling pathway cause complexity in this synapse as well as delayed sleep-phase syndrome.
Environmental factors:
- Prenatal viral infections: causes early fatal brain development, which can be linked to a higher risk of autism. The outcome of exposure depends on the maternal immune system and developmental stage of the fetus. Examples are: prenatal influenza, rubella, and cytomegalovirus infections.
- Zinc deficiency: it is necessary to have metal ions homeostasis for proper brain function and its disruption is linked to neurological symptoms and cognitive disease.
- Maternal diabetes: diabetes of the mother during pregnancy can be a risk factor for development of autism in offspring.
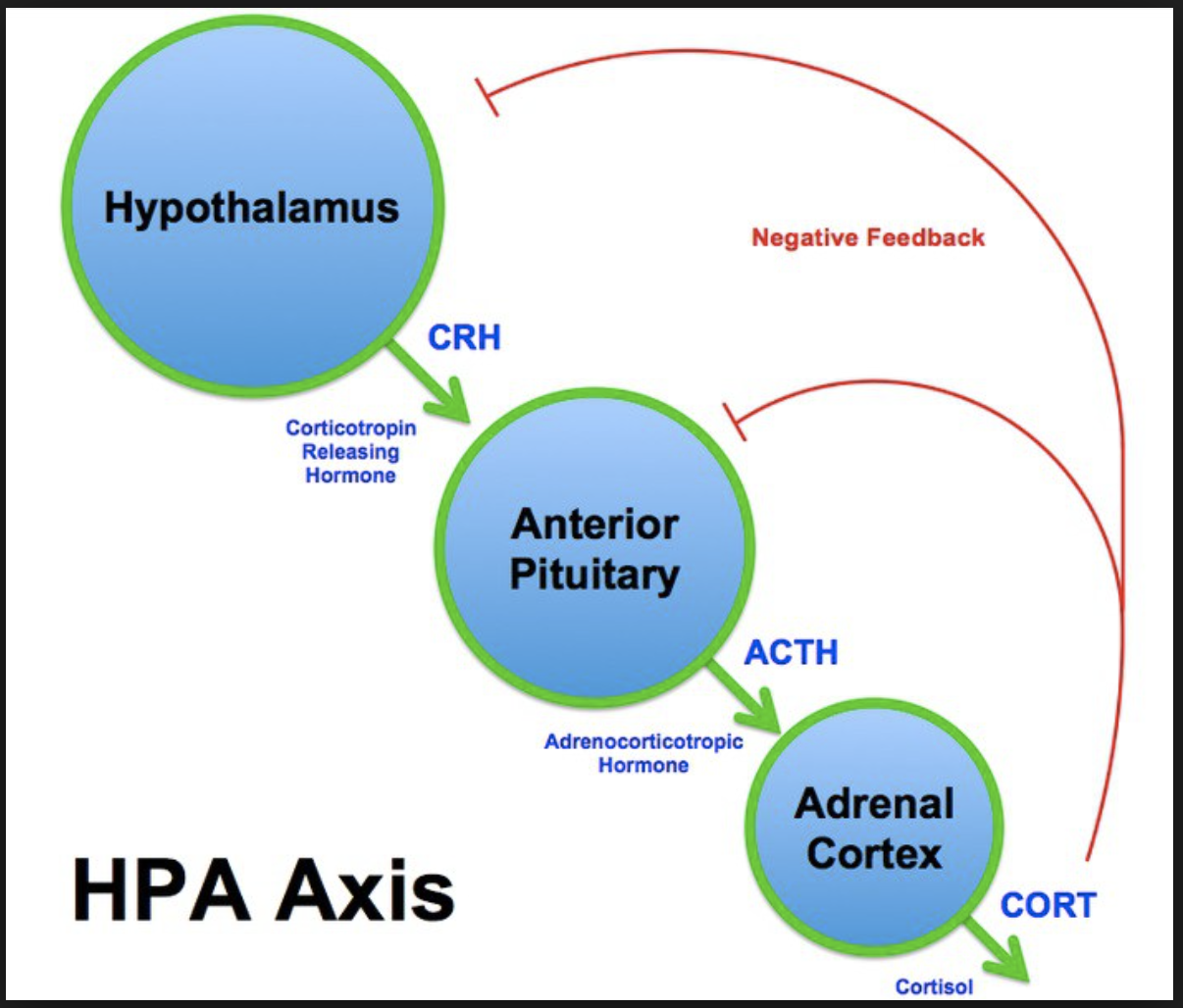
- Prenatal and perinatal stress: exposure to either stress hormones or psychological stress of the mother in are associated with greater risk of autism in offspring.
- Toxins such as prenatally exposure to valproic acid
- Parental age: studies indicate that advanced age of both mother and father is a risk factor for autism.
Vaccination?
After discussing the risk factors leading to autism, the important question of whether or not to vaccine is among many families in the society. There are many people who are strongly against vaccination. The unfortunate feelings of mistrust between the physicians and parents can be sensed to some extend among those who are against vaccination. As we discussed in our group, the physicians can make a difference in improving the situation by spending more time with the patients and speak about the benefits of the vaccines and educate the parents who bring their children to them. Having vaccination for autism mandatory in order to be able to attend public schools was also explored in our group. Such regulations takes away the right of making decision about health care from individuals. We also spoke about the importance of having autistic children in the same classrooms with other student. It is critical because it helps autistic students to interact and learn socializing skills. It also helps other students to develop friendship relationships with autistic students and become exposed to autism. This helps them to interact and develop skills, which can help them in their future lives as individuals who are going to take on jobs and live in the society.