Autism is yet another condition we discussed in class that I was not complete familiar with. I have met several people with autism of varying severity but I never really knew what may have caused it or what exactly was going wrong.
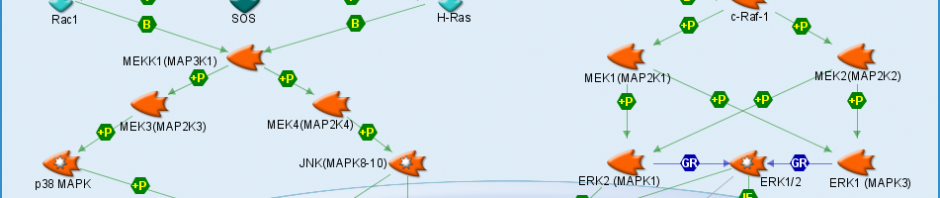
It turns out that my initial impression that autism was just one condition was incorrect. It turns out that autism is what is called a spectrum disorder meaning that it is several different pathways with similar outcomes combined to result in one condition. I was very surprised to find that so many different pathways were contributing to the symptoms typical of autism. Some neurotransmitters and receptors are present in smaller numbers than usual while chemicals leading to oxidative stress are at higher levels than usual.
The causes for autism seem to be a little hazy but genetics definitely seems to affect whether or not one develops autism. A genetic predisposition does not, however, mean that one will develop autism. Other environmental factors known as xenobiotics seem to also contribute to autism. Xenobiotics are basically anything put into your body that isn’t either made there or used fr nutritional purposes. Autism is generally diagnosed before the age of 3 or 4 and it is thought that those with the genetic predisposition that are then also exposed to some set of environmental factors very early in life will then develop autism.
It was widely believed for a period of time that infant vaccination was contributing to an increase in autism diagnosis. This belief was later found to be untrue but it is still believed that there is some outside contributing factor to the development of autism. Another possible reason for the increase in the diagnosis of autism is the awareness of both doctors and parents. Parents who are aware of the symptoms of autism are more likely to bring their child in for diagnosis where before the symptoms were widely known mild cases of autism may have just been written off as a little odd.
Researchers also believe that it may soon be possible to in part prevent autism in infants. They believe that identifying those with the genetic predisposition for autism will help parents and doctors avoid any adverse environmental factors as well as begin social therapies at a very early age while the parts of the brain responsible for social interaction are still extremely plastic. This combination is hoped to possible prevent some cases of autism and significantly decrease the severity of others.
Autism: Are the pieces falling together?