
Autism is more common today than ever before. According to the Autism Science Foundation, prevalence of autism was reported as 1 in 10,000. During the nineties, it decreased to 1 in 2,500 and eventually 1 in 1,000. In 2012, the Centers for Disease Control and Prevention cited the occurrence at 1 in 88 (see http://autismsciencefoundation.org/ for more information about autism). These rates have increased for several different reasons. Classification criteria have changed, technology in diagnosis methods have become more sensitive, awareness of the disease has increased, and parents have become more engaged in their children’s diagnosis process. Autism is diagnosed and treated along a spectrum. The causes, symptoms, diagnosis, and treatments for individual cases of autism can be quite varied, thus autism is often referred to as a spectrum disease. Recently, Asperger’s syndrome was repositioned underneath the umbrella of autism. An individual with this form of autism would experience life quite differently than an individual with autism in which development delays in areas such as cognition and language are key characteristics.

With the increased visibility of autism, many people have become more understanding of individual behaviors. Society today is putting more emphasis on awareness about numerous diseases, autism included. Increased awareness corresponds with an increased sensitivity to the issues individuals have and the needs associated with these issues. Inappropriate behavior in class or other socials situations would normally garner a matching social consequence. Usually, disciplinary action or another negative reaction would be the typical result. Special provisions and protocols may be put into place for those with social and neurological disorders. This sets the precedent for different social behaviors in response to irregular behavior that is due to a condition such as autism.
Like many other disorders, autism is thought to have both a genetic and environmental component that predisposes someone to be at risk for developing the disorder. In the article we read on autism, it was hypothesized that a variety of environmental factors can cause oxidative stress at the cellular level. These environmental factors, however, do not affect all individuals the same. Oxidative stress results only for those who are genetically vulnerable. This is a relatively small set of individuals compared with the population as a whole. Oxidative stress results in problems with methylation which affects genetic expression, resulting in delayed development and, in some cases, autism as well as dopamine receptor action that results in decreased neuronal synchronicity impairing attention and cognition, a hallmark of autism.
As diagnosis methods become more precise, more knowledge about the individual at the molecular level is gained, and helicopter parents become more perceptive to the medical needs of their children, increases of neurological disorders are being observed across the board. The question is ever more becoming, How will we define normal? Will each individual that has even the slightest deviation from the genotypic norm be classified as having a disorder? With so many variants and possibility for differentiation within our species, it seems that at one point or another, each of us must surely be abnormal once we look hard enough and to the most specific degree. I believe that what counts the most is how our idiosyncrasies affect the quality of our daily life and functioning. When a biological abnormality results in an inability to function as one desires, many believe this is what legitimates taking an action to reverse these effects through medication, therapy, or other means.
More Than Just Social Drinking?

Culture plays a role in the use of alcohol. Alcohol serves as a social lubricant, as it has across different cultures and time periods. Although alcohol appears as a common thread in the tapestry of varying societies, its expression may differ from place to place and time to time. This social practice has the profound ability to affect one’s health, either for the better or the worse. While some drink alcohol for its immediate effects, prolonged usage can affect the neurological wiring of the brain. The driving force for drinking changes, and metabolic processes can become affected. While genetic predispositions and personal behaviors certainly play a large role, the role of society and culture should not be ignored.
In class conversation, we discussed the role of alcohol in our own community. Fargo-Moorhead is a community that supports alcohol and enables those that are especially susceptible to alcoholism. As a college community, the bar industry definitely appeals to the college demographic. This community has specials unlike any community I have ever heard of. On any given night, one could find a bar selling drinks for $2.50 and much less. Friday nights at the Old Broadway: 2 hours of 10 ounce draft beers for the same cost in pennies as the date. Bucks and The Bar give away 40 and 48 ounces, respectively, of almost any beverage (beer, mixed drinks) for free, weekly during the month of one’s birth. Many bars have set up text clubs to inform their patrons when their specials are. Bars give away free shots at the door when special texts are shown, advertise trips to Vegas, 70” TVs, and other events to lure individuals to their establishment. Big D’s advertises 2-4-1 and for an extra dollar, a third drink. Mug nights, dollar-you-call-its, and the list goes on. Not only does our society support drinking, it supports binge drinking. With an age limit of 21, drinking in America has turned into something that is done irresponsibly in secret until they are legal and something one does in great excess once they become legal.

We also discussed countries where the legal drinking age was lower and alcohol was integrated into culture more than in the United States. In Italy, it is common to have an alcoholic beverage with dinner nightly. When used in moderation, such as in this instance, alcohol can actually be healthful for an individual, including reduced risks of coronary heart disease, type 2 diabetes, and some types of cancer. In Ireland, the institution of the pub is a pit-stop between home and work for many. This practice is somewhere between the Italian and American examples. While college American culture exhibits occasional to frequent binge drinking and Italian culture exhibits a single frequent, if not daily, drink, the Irish example appeared, to us, to be an example of frequent, if not daily, moderate drinking.

Even at the level of minimal drinking, the brain is affected. Receptors associated with reward are stimulated, so the individual feels the effects of ethanol to be positive ones. The body’s inhibition system is compromised, and the feeling can be quite liberating. Ethanol literally enables a different state of mind for those consuming alcoholic beverages. Prolonged use and abuse of alcohol, however, can damage the body. By stimulating the same parts of the brain with great repetition, one begins to develop a tolerance to ethanol. Higher levels are needed to attain the same level of reward in pleasure centers of the brain. Acetaldehyde, a product of breaking down ethanol for use by the body, alters the cell at the molecular level and can change which genes are turned “on” and “off” by transcription factors.
In addition to the problems alcoholism itself can cause, the number of diseases that exist in comorbidity with it is cause for great pause. Although used as self-medication by many, alcohol use can actually aggravate other mental health problems. Socialization and cultural norms are important in the decisions individuals make and the impact those decisions can have on one’s health. Alcohol is a drug that has the capacity to affect and change the way the mind and body function. When it comes to consuming alcohol, moderation is key, no matter what the cultural norm tells you.
Capstone? What's a capstone?

At the start of the semester, other than knowing I had to take a capstone course in order to get my degree, I had absolutely no idea what I was getting myself into. Little did I know, the neurochemistry capstone that I had signed up for would become one of my favorite courses I’ve taken in my college career. Not only was the material very interesting, but the style of the course was entirely different from any other course that I had previously taken at Concordia and was in fact very favorable for learning.
Prior to taking this class the normal class structure that I had participated in consisted of lecture style teaching with around four tests and some quizzes thrown in the mix. Neurochemistry was an entirely different class, as it prompted discussion and problem solving from the students as we explored a vast array of neurochemistry related topics ranging from neurodegenerative diseases to alcoholism. We started the course by exploring a different neurochemistry topic each class period and submitting information that we found onto an online page so we could learn the material cooperatively as a class. Once we learned the basics of neurochem we started diving into scientific papers that dealt with different disorders and used problem-solving skills to dissect the papers and obtain a common understanding of the topic. We finished each week with a class discussion about each paper that engaged everyone’s thoughts and opinions as we discussed each paper. I thought this was a very nice change as it prompted us to learn the material because we wanted to learn it rather than learning material that we weren’t as interested in. It was also very nice to be in a relatively small class that was very comfortable with each other so we could easily share our opinions and present new material that we had learned with the class.
My favorite part of the course was the fact that we tied each topic into our society. This made the topics much more interesting because we could relate to each different point and talk about how we thought each disorder affected our society as a whole. Simply due to this fact we were definitely practicing Concordia’s liberal learning concept known as BREW, or becoming responsibly engaged in the world. Throughout the whole class we looked at different disorders that affect the lives of many individuals in our society in an attempt to understand just what neurochemical processes were flawed and if there would be any way to cure the disorder.
Overall I thought this was a great course for so many reasons. It is one that will definitely be helpful in the future as we go out into the world and engage in society and are forced to use our problem solving skills in order to make the world a better place. This class definitely developed my problem solving skills, as well as my ability to be able to communicate very complex information in an understandable manner. All in all the capstone experience was a great one!!
Is the complex world we live in a possible cause of the rising cases of autism?

Our final neurochemistry topic of the semester focused on the developmental disorder known as autism. Autism is a very interesting topic because its cause can be due to so many different events and it is relatively hard to get a concrete diagnosis. The general definition of autism states that it is a disorder of neural development characterized by impaired social interaction and communication. The paper that we explored outlined two particular hypotheses for the cause of autism, looking at both the genetic factors as well as the possibility of different environmental factors present in the causing of autism.
The world that we live in is becoming increasingly complex as science develops new ways to build different products with new materials that often contain both heavy metals and xenobiotics. Xenobiotics are simply chemicals that people can come in contact with and the main heavy metals that our paper focused on were arsenic, lead, and mercury. Combining these heavy metals and xenobiotics with genetic predisposition there is an extreme risk for the development of autism. I will start out by briefly describing the science behind the hypotheses outlining the development of autism. The development of autism starts out with either genetic factors or the exposure to heavy metals and xenobiotics causing impaired sulfur metabolism. This impaired sulfur metabolism then inhibits the activity of methionine synthase causing decreased methylation of DNA, ultimately resulting in developmental delay and autism.
One of the main topics that we talked about in our discussion dealt with diagnosing autism and what this does to the social status of a child. Diagnosing autism can be very difficult because the symptoms can cover a very broad spectrum ranging from very severe to very minor. It is very hard for parents to know when to take their children into the doctor to get examined because it’s hard to know for sure if your child is simply in an awkward stage of development or is in fact suffering from the developmental disorder known as autism.
I personally have a family friend who was diagnosed with Asperger syndrome, which is an autism spectrum disorder that is very similar to autism but can be less severe. In my friend’s case, he had a very awkward childhood and struggled socially prompting his parents to take him to the doctor, ultimately to be diagnosed with Asperger’s. He now has grown up substantially and if you didn’t know that he had been diagnosed it would be impossible to tell that he has an autism spectrum disorder but he will forever have the title of having Asperger’s. This is just one example showing the difficulties of diagnosing autism spectrum disorders and how hard it must be to label a child with autism.
It will be very interesting to see whether or not the number of cases of autism will continue to increase at the rate it is today now that scientists are uncovering more and more information on the causes of autism and whether or not they will be able to come up with a way to either prevent autism or treat individuals that are already suffering form the developmental disorder.
Liberal learning at its finest: Concordia College Neurochemistry
 In a typical class for a core requirement at Concordia College there is usually a new perspective, a new skill, a new set of knowledge, or even a new language is learned. In my studies in chemistry I would not expect to learn the theologies of Islam, ancient Greek myth, or the development of the medieval castle in Europe but I was surprised to find great interest in these subjects and many others. The liberal arts learning have instilled in me a love for learning as is the first goal of liberal learning at Concordia. To top off the liberal arts major we must take a capstone class in a topic of our choice. I chose to take Neurochemistry as it related to my major field of study. This class has been stimulating and challenging and I am grateful for the opportunity to take it.
In a typical class for a core requirement at Concordia College there is usually a new perspective, a new skill, a new set of knowledge, or even a new language is learned. In my studies in chemistry I would not expect to learn the theologies of Islam, ancient Greek myth, or the development of the medieval castle in Europe but I was surprised to find great interest in these subjects and many others. The liberal arts learning have instilled in me a love for learning as is the first goal of liberal learning at Concordia. To top off the liberal arts major we must take a capstone class in a topic of our choice. I chose to take Neurochemistry as it related to my major field of study. This class has been stimulating and challenging and I am grateful for the opportunity to take it.
The class does something that most others do not, we stick our heads out into the scientific community and grasp onto multiple subjects trying our best to understand them. This is a skill that I will need for my career as I will be reading and writing the same type of scientific publications we tackle. Not many classes are able to provide this type of experience as they rarely peek out of the textbooks and assigned book readings mostly because the other core classes are at the 100 to 200 level, basic classes. Neurochem throws us into a world without a textbook causing us to learn for ourselves, be resourceful, and depend on each other as a team to understand the complex publications that we read. We cannot simply refer to the textbook to solve a problem or solidify a concept we cannot understand because these papers are often illustrating cutting-edge research that has yet to be recorded in texts mostly because even the researchers are not 100% confident their conclusions are the correct answer to the problem. This allows us to also form opinions when we can look at multiple hypotheses relating to one subject. This helps me for my career in chemistry as I will have to form my own hypotheses about new projects that I will undertake as a graduate student and beyond.
What I really enjoyed about my capstone experience is the component of learning from my peers. Every week we dissect a paper and assign different sections that the class is struggling to understand to each person in the class. Then we come back in a few days and present what we learned after researching the topics assigned to us. Through this technique we are learning from each other’s interpretation of the material and therefore it has been simplified and summarized so we may understand it better. This will be something that is very helpful to multiple careers as it will most likely come up that we will have to present some information, reports, etc. to our colleagues and peers.
Overall, the class has been a great experience in teaching me new material in a new way, broadening my learning abilities, perspectives, and knowledge base. I have come away with greater analytical skills and the ability to dissect complex topics into simpler terms in order to understand them and move forward.
Animal models used to study alcoholism: What can we learn?
 In many different areas of science, animal models are used to begin understanding of diseases and behaviors analogous to humans. This animal model concept has also been used in the understanding of alcoholism and behaviors associated with alcohol consumption. Researchers have found that there are essentially three phases of alcohol consumption: acquisition of drinking alcohol, controlled alcohol-drinking behavior and uncontrolled alcohol-drinking behavior. It is agreed upon that this is a working progression model for alcoholism. Within it are transition phases as well that deal with biological, psychological, and social vulnerability factors. Most studies have only looked at the first phase of this model but more recent works have revealed information about the second and third phases.
In many different areas of science, animal models are used to begin understanding of diseases and behaviors analogous to humans. This animal model concept has also been used in the understanding of alcoholism and behaviors associated with alcohol consumption. Researchers have found that there are essentially three phases of alcohol consumption: acquisition of drinking alcohol, controlled alcohol-drinking behavior and uncontrolled alcohol-drinking behavior. It is agreed upon that this is a working progression model for alcoholism. Within it are transition phases as well that deal with biological, psychological, and social vulnerability factors. Most studies have only looked at the first phase of this model but more recent works have revealed information about the second and third phases.
In a long-term study, researchers exposed rats to varying concentrations of alcohol (5, 10, and 20%) for a 10 month period. During this time, the rats were exposed to the alcohol for 2 months and then deprived of it for 2 months and so on. These rats settled into an alcohol consumption pattern of 4 g/kg for a day and a preference of 5% alcohol. After a time of alcohol depravation the rats experienced a significant rise in alcohol intake (from the normal 4 to 6 g/kg) and preference (higher concentrations, 10 and 20%), this is termed the alcohol depravation effect (ADE). The rats experiencing the ADE not only consumed more alcohol but developed a preference for the higher concentrated alcohol solutions. This was paralleled with a development of increasing consumption of alcohol at inappropriate times of the day in an uncontrolled and compulsive manner. Rats normally stay dormant during the day and partake in minimal activities and being more active during the night hours. The rats began to consume alcohol during light hours and dark hours disregarding normal circadian schedules. This study also found that anti-relapse drugs were able to dampen the ADE so as to decrease the likely hood of increasing alcohol need/want behaviors after relapse.
Despite the strangeness of giving rats alcohol and studying them this study has high relevance to our consumption behaviors and possible treatments. The rats that began drinking more alcohol and at higher concentrations so are now considered to be in a state of uncontrolled alcohol-drinking behavior. Their transference into this stage from controlled alcohol-drinking shows that there are addictive properties to alcohol that need to be addressed with treatment and thus their development of treatment of the rats may be applied to humans with further study. Struggling alcoholics could be given a pill to slightly or completely diminish their psychological need for alcohol.
Another study introduces the reinstatement model for alcohol-seeking behavior. Here, an animal is trained to self-administer alcohol and is then subjected to extinction processes to extinguish the operant conditioning that had been established. Researchers found that the reinstatement of the behavior can be easily renewed with administration of a very small amount of alcohol increasing the subject’s craving by a great deal. This reinstatement model is widely accepted. Studies using this model have suggested that the neuronal substrates mediating alcohol-, stress, and cue-induced reinstatement are not identical. So, more than one neurobiological pathway is linked to provoking alcohol-seeking behavior. This has been shown pharmacologically when different treatments treat different associations made with alcohol. The reinstatement model is therefore used in developing new drugs to fight craving for alcohol.
Autism: Are the pieces falling together?

Autism is yet another condition we discussed in class that I was not complete familiar with. I have met several people with autism of varying severity but I never really knew what may have caused it or what exactly was going wrong.
It turns out that my initial impression that autism was just one condition was incorrect. It turns out that autism is what is called a spectrum disorder meaning that it is several different pathways with similar outcomes combined to result in one condition. I was very surprised to find that so many different pathways were contributing to the symptoms typical of autism. Some neurotransmitters and receptors are present in smaller numbers than usual while chemicals leading to oxidative stress are at higher levels than usual.
The causes for autism seem to be a little hazy but genetics definitely seems to affect whether or not one develops autism. A genetic predisposition does not, however, mean that one will develop autism. Other environmental factors known as xenobiotics seem to also contribute to autism. Xenobiotics are basically anything put into your body that isn’t either made there or used fr nutritional purposes. Autism is generally diagnosed before the age of 3 or 4 and it is thought that those with the genetic predisposition that are then also exposed to some set of environmental factors very early in life will then develop autism.
It was widely believed for a period of time that infant vaccination was contributing to an increase in autism diagnosis. This belief was later found to be untrue but it is still believed that there is some outside contributing factor to the development of autism. Another possible reason for the increase in the diagnosis of autism is the awareness of both doctors and parents. Parents who are aware of the symptoms of autism are more likely to bring their child in for diagnosis where before the symptoms were widely known mild cases of autism may have just been written off as a little odd.
Researchers also believe that it may soon be possible to in part prevent autism in infants. They believe that identifying those with the genetic predisposition for autism will help parents and doctors avoid any adverse environmental factors as well as begin social therapies at a very early age while the parts of the brain responsible for social interaction are still extremely plastic. This combination is hoped to possible prevent some cases of autism and significantly decrease the severity of others.
Ethanol: A matter of perception?
As we discussed ethanol this week in class I began to realize that the problem with alcohol in our country is truly a problem of perception. I’m not saying that we perceive the problem as larger than it is, but I do believe that our perception of alcohol as well as our perception of those who use it in excess is contributing to the problem.
Under aged drinking is obviously a problem we experience on a regular basis. It is rampant in colleges, universities and many high schools across the country and it seems that when those who are under age as well as those in college drink to excess when they have the opportunity. Solutions range from stricter enforcement to a lower drinking age to a flat out prohibition but I think our problem has a simpler solution. Change the perception of alcohol. Growing up you hear from your parents that alcohol is for adults and that you should never drink it until you are an adult. Right away you get rebellion and a desire to be an adult driving under aged people to want to drink. Next you have the Jersey Shore and other shows and movies that show people getting completely hammered and having tons of fun doing it. This sends the message that the purpose of drinking alcohol is to get completely smashed. If we could change how the consumption of alcohol is portrayed both in the home and in the media I think the urge to drink and drink to excess would decrease among under aged people.
Habitual and excessive drinking can also lead to the other perception I consider to be incorrect. Most of society view alcoholics as lazy slobs who are running away from their problems but chose not to help themselves. While it may be true that the initial drinking may have been in response to emotional stress, it is not likely the reason they continue to drink. Alcoholics develop an addiction much like any other drug addict. Ethanol affects many pathways in the brain some of which cause the lowering of inhibitions and slowing of cognition. Ethanol also causes the release of dopamine, the “happy” neurotransmitter, in regions of the brain that are related to behavior reinforcement. So just like your dog doing a trick to get a biscuit, alcoholics drink to get that rush of dopamine. They should be treated just like any other addict. Many alcoholics do not seek help because of the social stigma attached to alcoholism. If they were encouraged to get help and praised for getting healthy like those with other addictions they would likely be more receptive to help.
If these perceptions about alcohol and its use could be altered then I believe we would see a shift in the way it is consumed without have to change laws. Other countries have similar laws in place but do not experience the same problems because drinking alcohol is portrayed as something that is normal in moderation and is not meant to be consumed exclusively by adults in a party type setting.
Bipolar: You may not have even known.

Before our discussion of bipolar disease in class I always imagined people who would seem fine one second and then have a huge, angry outburst. I genuinely believed that the emotions of people with bipolar could turn on a dime. I was once again proven to be wrong.
Bipolar disease is long periods of depression followed by long periods of mania or hypomania (an emotional state in which the subject is extremely happy but not manic). Hypomania is more difficult to diagnose because it seems more like a peppy personality than a chemical imbalance. The exact pathway causing this imbalance is not known which makes you start to wonder how exactly medications are made and prescribed for this disease.
The most common method of prescription for bipolar is called rational pharmacy. Basically what this means is the doctor will prescribe the patient a drug depending on the symptoms they are experiencing at the time. If the patient is exhibiting depressive behavior they are prescribed an antidepressant and vice versa. There are very few drugs that are very effective for the manic stages of bipolar so it is the depression that is primarily treated in most patients anyway. This method often requires trial and error which can cause patients to be without proper medication until the correct mix of medications is found.
I find this fact to be a rather unfortunate one, but despite not having any idea what the cause of the disease is or how exactly to treat it there are many people who are very well known and constantly in the public eye who deal with bipolar without letting on that they have it. Some of these people include Russell Brand, Robert Downey Jr., Mel Gibson, Amy Winehouse, and Catherine Zeta-Jones.
Concussion: An unknown threat.
I am, like many other people, a student athlete. I have been playing rugby since I was 14 years old and the topic discussed this week in class took me quite by surprise. As an athlete at the age of 22 still engaged in a full contact sport I had no idea what exactly what a concussion was. I have myself suffered from a concussion on more than one occasion but I never thought very of them. I had always had the impression that they were sort of like a small brain bruise. Painful and annoying, but temporary with no lasting effects. I could not have been more wrong!
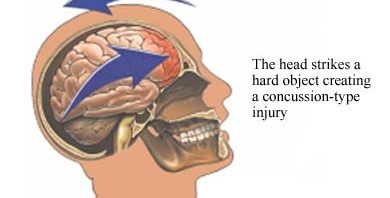
When you suffer a blow to the head or your head is caused to stop suddenly your brain also receives much of that force. This force causes the brain to move, stretching neurons. As the neurons are stretched various neurotransmitters effectively get squeezed out of them, sort of like twisting and stretching a wet wash cloth. The neurotransmitters that are rapidly released can cause swelling, increased blood flow, and even minor cell death. It also can cause confusion when signals are being sent through the injured part of the brain. These are what cause the characteristic headache, nausea, and mild amnesia associated with concussion.
That information alone changed my view on concussions enormously but there was even more to learn. The imbalance of neurotransmitters is not something that the brain can clear up quickly. Residual imbalances can last for weeks and recovery time varies depending on the person. During the recovery period those who have suffered a concussion should not only cease physical activity until cleared by a doctor but they should also limit the strain they put on their brain academically. After a concussion strenuous use of the brain like reading for extended periods of time can exacerbate the problem and cause headaches. Children take more time to recover from concussions than adults do which I thought would have been the other way around. Also if an athlete returns to play before the concussion has healed completely there is a significantly greater chance that they will suffer another, more severe concussion. There is also a chance that the athlete could suffer a very rare injury called second impact syndrome which can cause death within minutes of the second impact.
As an athlete who has participated in a contact sport for many years I felt that I should have been more aware of what exactly a concussion was. Having suffered multiple myself, one of which was rather severe (my nose was broken and two of my front teeth were knocked out), I would have liked to know that perhaps I shouldn’t have been doing some of the things I did afterwards. The concussion occurred on a Sunday afternoon and I was back in school on Tuesday and back at practice the following Monday. The rule for my league was I only had to sit for a week so long as my doctor cleared me and I felt OK to play. At the time I felt just fine but I feel like I may have made a different decision if I had known more about what was going on.