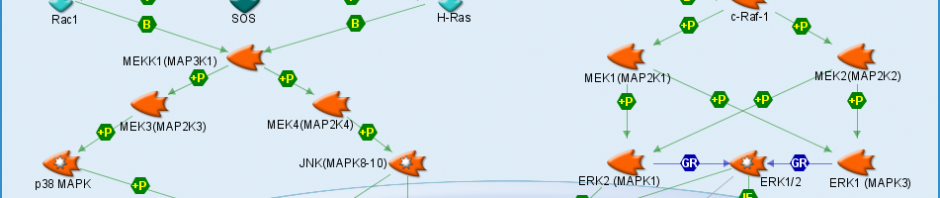
The MAPK pathway is incredibly important in our brain. Its functions range from cell growth and development to inflammation and cell death. This pathway is incredibly large and is responsible for many different things. Diseases like Parkinson’s and ALS have been linked to a disruption in the MAPK pathway leading to oxidative stress.
Oxidative stress occurs when oxidant by products from certain processes reach levels that are too high for cells to deal with. The stress placed on the cells can be relieved but if it is not it affects how well they are able to function and can even lead to the death of the cell. It is believed that those with neurodegenerative diseases like Parkinson’s and ALS are experiencing motor neuron deterioration due to oxidative stress.
Targeting the MAPK pathway to fix this is problematic. Because MAPK is important to so many other processes it is almost impossible to alter it in a way that would prevent Parkinson’s or ALS and not cause some other problem in a different part of the pathway. The use of stem cell therapy has been used in an attempt to replace the lost motor neurons. This treatment appeared to be working for a time as the stem cells developed into new motor neurons but shortly afterwards the oxidative stress caused those neurons to degenerate just as the first ones did.
Neurodegenerative diseases like Parkinson’s and ALS are crippling to those who have it as well as those around them. Research is trying to find ways to make drugs that will target extremely specific receptors in the hope that being able to do so will make treating diseases like this possible when it has been impossible in the past. The number of important function performed by the MAPK pathway is too large to try and alter it without very target specific drugs.
The following is a link to a diagram of the MAPK pathway: http://www.avivasysbio.com/research-areas/mapk-signaling-pathway
We all know that sweets and fast food are bad for our health. They rot our teeth, add inches everywhere we don’t want them, clog our arteries, and put stress on our heart, but do they also affect our brain health? Current research is suggesting that yes, eating an unhealthy diet can, in fact, cause problems for our mental health.
Many of us are aware of the increasing rate of type II diabetes in the U.S. Type II, unlike type I, is caused by insulin resistance. Basically insulin is responsible for getting glucose into cells to be used for energy. When your body becomes resistant to insulin the glucose is not properly transported. Because the glucose is not reaching the cells your body thinks it still needs that energy so your liver produces even more glucose into your blood. Again the glucose cannot be taken anywhere so it builds up in the blood, a condition called hyperglycemia. This condition can be managed relatively easily with medication. What was not known about insulin resistance until just recently was that it can also occur in the brain.
Glucose is the primary form of energy used by the brain. Researchers are finding that in Alzheimer’s disease there is reduced use of glucose in parts of the brain. If the brain cells aren’t using as much energy then they are not working as well as they should be. It is believed that brain cells are also capable of developing insulin resistance so glucose is not properly transported to the cells that need it to function correctly. This is what is believed to be causing the progressive memory loss associated with Alzheimer’s.
If insulin resistance is such a large part of two very common problems what causes it to happen and how can it be avoided? Insulin receptors can become less sensitive to insulin levels if insulin levels are chronically high. Since cells only need as much glucose as they need to produce energy the insulin receptors need to become less sensitive if there is regularly more insulin present than the cells need to import glucose. This occurs when a diet is full of unnecessary sugars and fats that are most often present in sweets, sodas, and fast food. If this life style is maintained overtime the insulin receptors can become resistant to insulin and that can lead to type II diabetes and even Alzheimer’s disease.
I am not trying to say that if you indulge in a Big Mac or a can of your favorite soda from time to time you are going to develop diabetes or Alzheimer’s disease. Moderation is always key and an unhealthy diet does not guarantee that you will develop one of these conditions. Awareness of how your food choices will affect you now, tomorrow, and 20 years down the road is important and knowing the cause of diseases like these can help in future treatment options as well as prevention.
The legal use of marijuana has been a hot topic in the U.S. for years. The primary argument for its use is that it has shown to be highly effective for those suffering severe pain. The use of medical marijuana is legal in many states, but is the use of medical marijuana truly necessary? Are the benefits of its use greater than its drawbacks? What if there was another option?
Marijuana works as a pain killer by working in a system called the endocannabinoid system. When compounds like cannabis are present in our body they bind to our neurons and decrease the amount chemicals that are released from these neurons. At the site of an injury or other source of pain the chemicals being limited are those that would cause sensitivity and inflammation. This is why medical marijuana is used to reduce pain and why it is so effective.
The obvious drawback to the use of marijuana is its psychotropic or mood and behavior altering effects on those using it. THC is the primary chemical found in marijuana. While it does relieve pain it also causes mood and behavior changes as well as other side effects including increased appetite often referred to as “the munchies”. A synthetic form of THC is available as a prescription in both the U.S. and Canada under the name Marinol.
A lesser known component of cannabis is Cannabidiol. Cannabidiol makes up about 40% of the compounds present in cannabis and functions in much the same way as THC. The major difference between the two is that Cannabidiol does not have the psychotropic effects of THC.
Knowing this is there truly any reason for the use of medical marijuana? The main components present in marijuana can be made synthetically in a lab and the non-psychotropic component can be separated from the psychotropic one meaning we can have the pain relieving effects of marijuana without any other side effects. Also if the medically significant components or marijuana are produced in a lab instead of being grown either in or outside of the United States the rate of abuse would likely decrease because anyone with possession of the plant based form of the drug would be in violation of the law. Also Cannabidiol would not be abused as a recreational prescription because it lacks the psychotropic effects sought by a recreational user. On a whole the use of medical marijuana is becoming unnecessary as more is being discovered about the chemical components and how they can be synthesized in a laboratory setting. In addition the synthesis of these drugs would make distribution, possession, and growing laws much simpler for those truly using the drug for medical purposes and for law enforcement. On a whole unless you are looking for a high there is no reason for the legalization of marijuana.
For those of you who can’t read 0.2 size font, the molecule shown in the featured picture is oxytocin. Eh? Eh? Get it?
Anyway, this course truly was everything I wanted and more. Unlike many of my classmates, I took Neurochemistry as basically the only elective I will be able to take in my undergraduate career. (Filling requirements for a chemistry major, a math major, and all the liberal arts core classes that a Concordia degree requires takes quite a bit of time to complete without overloading or going insane.) Actually, during my sophomore and junior years I considered dropping my math major to pursue more coursework in neuroscience, thinking that ultimately I’d go to graduate school for neurochemistry. Thus, discovering that the neurochemistry class offered here fit into my schedule my senior year, I was pretty darn ecstatic. However, I noticed that the class did not have a lab associated with it which was different from any science class I had taken, so I was a bit wary of what would be in store, especially since it was attributed as a senior capstone class. Capstone classes are, by definition, writing-heavy classes, and writing papers is not one of my favorite things to do, to put it lightly. I want a word that means frustrated but none of the synonyms suggested by Word are the one I’m thinking of. WHAT IS IT??…. Oh. I guess “frustrated” works.
Despite my pre-semester concerns, however, this class turned out to be not only enjoyable, but extremely useful as well. I think that one of the weaknesses of the chemistry classes I have taken thus far is that they don’t take much time to connect the course material with what is actually happening in the field. Granted, most just don’t have the time to do this due to the tremendous amount of material that needs to be covered in a short time, but it is still very important to those that are going to do research at any time in their chemistry careers. From my summer undergraduate research program, I have discovered that reading these sorts of articles comprises an almost unbelievable portion of one’s time spent in research. A person needs to gather foundational information on the material and instrumentation to develop a method for their project, make sure that someone hasn’t already done the same experiment, and in some cases search literature for an initial topic that is important to the scientific community. This course not only encouraged reading scientific articles and reviews, but the required reading was solely these articles. Scientific journals are a very different form of writing than most prose, and in order to read them fairly quickly and effectively, a person needs practice. With our weekly journal articles, we both gained familiarity with this style and learned how best to go about dealing with the information presented. Each week we worked together to understand the overall message of the article, determine what was important and what was trivial, and communicate our findings with the non-science world. This last portion is the reason for this blog series, and definitely an important step in the research process; although it’s necessary to effectively communicate with the rest of the scientific community, it’s extremely important to share our progress with the rest of society to gain support and feedback to continue or reevaluate different aspects of a project. Working within a fairly specific group of probably like-minded people, one’s perspective can easily become skewed; communication with other groups helps to ground oneself. I still think this is a good idea…
This class has been so beneficial to me that I would suggest that it become part of the required curriculum for an ACS Chemistry major. For a person going into research, learning how to process information from scientific journals is a necessity and something that isn’t really done in any other chemistry class. Peer discussion on research was also emphasized, which is unlike other courses, yet essential to most jobs in the field. This course has, in short, most strongly conveyed the link from my undergraduate studies to skill application in the field than any other course I’ve taken. I recommend it to any and all science majors. It’s fantastic.
It shouldn’t come as a surprise to hear that obesity is one of the most prevalent medical concerns in the United States. In fact, 30% of the US population has obesity and 30% of these individuals also has diabetes. Our society is a point where the number of cases of type 1 diabetes in young people under the age of 18 is increasing. In order to combat this rise in obesity and diabetes regulations have been placed on fast food businesses, requirements such as food nutrition labels have been implemented, and grassroots campaigns against chemicals such as Red Dye and High Fructose Corn Syrup have sprung up around the country. These regulations have been put in place as an attempt to curb people’s eating habits and make them aware of just what they are eating. However, the issue of obesity and diabetes may not stem solely from society’s increased consumption of food. In order to understand the cause of these issues we must delve into the brain and observe the interactions of two chemicals: Leptin and Insulin.
While insulin is a term you’ve probably heard about, you may be unfamiliar with leptin. First, a brief summary of insulin. Insulin is a peptide hormone which regulates the amount of glucose taken in by cells throughout the body. Within the brain, insulin controls glucose intake by neurons, regulates acetylcholine, and contributes to memory function (http://www.hbo.com/alzheimers/science-insulin-in-the-brain.html). Similarly leptin is also a peptide hormone. Leptin is an important regulator of food intake (appetite) and body weight. In the brain leptin and insulin receptors are primarily found within the hypothalamus in a region known as the hypothalamic arcuate nucleus. Chemicals such as neuropeptide Y (NPY), agouti related protein (AgRP), and proopiomelanocortin (POMC), which are released based on leptin and insulin concentrations, cause the neurons in this region to be known as appetite-regulating neurons. When concentrations of insulin and leptin are high, POMC is released which reduces food intake and when concentration are low, NPY and AgRP stimulate food intake.
It might be helpful to know some of the Biochemistry of leptin signaling. Leptin stimulates cytokine receptors, which activate the JAK/STAT pathway towards gene expression. JAK, janus kinase, is a protein bound to the cytokine receptor, which upon stimulation of the receptor becomes phosphorylated. The phosphorylated JAK then creates a bind site for STAT (signal transducers and activators of transcription) molecules. STAT then enters the cell nucleus where it transcribes DNA for gene expression.
Now that some of the Biochemistry is out of the way, it is important to discuss how levels of leptin contribute to the rising levels of obesity in the US population. People with obesity have a flood of leptin in their system so the cytokine receptors become resistant to the overabundant leptin. This means that the appetite controlling chemical POMC is not produced because the neurons are not receiving leptin. Therefore, the signal stop food intake in never activated. On the other side of the metabolic disorder spectrum, people with anorexia have high levels of leptin without receptor resistance, thereby expressing POMC and preventing craving for food intake. Therefore, dyregulation and imbalance in leptin levels in the brain can cause various metabolic disorders such as obesity.
It’s hard to believe that it’s over. I’m not going to lie, I was nervous about this class knowing that it was going to be a good deal of biology, despite the neurochemistry name. Proteins, receptors, lipids, synapses…. As we say up here in Minnesota, ‘Ufda!’ I feel that I’ve grown in a lot of ways over the past semester.
The idea of a paper a week was very intimidating at first, but a 15 page scientific article no longer fills me with dread and foreboding (the last five pages are usually references anyway!) and my knowledge about the brain and how it works has definitely increased, although there wasn’t a lot there before, at least not a very in depth knowledge. I really appreciated coming together on Monday to a safe place and accumulate the things in the article that we did not understand. It made me feel less alone in the strenuous process of trying to get a basic idea of what the paper was talking about and gives a great method for getting deeper knowledge out of any paper that you read. Wednesday, or information day, when we all come together to give synopsis of the extra information dug up on subjects we didn’t fully understand always went quickly, but it was nice that if there was something that I missed it was on the wiki to be reexamined at a later time.
I think that Fridays were out “BREW” days (BREW is Concordia College’s motto ‘Becoming Responsibly Engaged in the World’). It was interesting to see everyone’s perspective on the subject as a health issue and how it relates to social issues, not just the pure science of it. More than that, it allowed us to reflect on science and its impact on society as a whole and moral dilemmas that occur within the scientific community.
On the whole, I have taken some new skills and improved other skills through this capstone experience. I have become better at reading and deciphering information from scientific papers as well as presenting that information in a relatable manner, both through the Wednesday information sharing sessions and through the blog posts. They say that being able to teach information is the best way to cement it in your own mind, and I cannot agree more. I think that this experience with scientific papers will help my own writing, better knowing what is expected in published papers. All in all, this class has been a good experience for me and I really appreciate the change in pace from so many other science classes that I have taken in the past.
To be honest, I took the class because it fulfilled my senior credits, capstone requirement, and elective course for my chemistry major. In the beginning of the semester, I thought this course would be an advanced biochemistry class with intense focus into neurochemical pathways. However, it turned out not to be the case. Instead of just throwing whole bunch neurotransmitters and the pathways to us, Dr. Mach taught the course in a much different way, a way that’s totally new to me.
Each week, we are required to read the “paper of the week” over the weekend, discuss the questions we have in class, and each of us gets to choose a specific topic to research on every Monday. On Wednesdays, we’d share the information we gather with the entire class including Dr. Mach. And on Fridays, the discussion leaders take over the class, host discussions on the topic of the paper and make connections between academic with the real world problems. After the discussions, we are required to write up a blog post online on our class blog. At first, I was not used to this discussion-based lecture style, but as the curse goes on, I realized the benefits of it. This type of teaching allows me to not only acquire the knowledge that normal lecture could provide, but also improve my research method, and ability to analyze scientific articles. Although blogging and creating a wiki were not the form of assignments I was used to (I’m not a blogging type of person as you have read), the fascinating topics really sparked my interest and making these assignments more than enjoyable.
The capstone course is an opportunity for us to demonstrate that we have achieved the goals for learning established by our undergraduate education. As a chemistry major student, this class allows me to apply what I have learned in the past 3 years to some of the most advanced researches. It also promotes the theme of Concordia’s core curriculum, “BREW”, Becoming Responsibly Engaged in the World. After all, although biochemistry is not my focus, I really enjoyed this class and hopefully I’ll be able to apply the skills I gained from this experience to BREW.
I’m going to be honest and say I took this class because it fulfilled two requirements for graduation. As a chemistry class, it has served as my elective course for my chemistry major. As a capstone class, it has served as my required core capstone for graduation. I also thought it would fit nicely as a bridge between my psychology minor and chemistry major.
Little did I know the things we learned would apply to my daily life and to my future career plans. I have noticed over the course of the semester being far more interested in what is going on with different diseases and disorders rather than simply how to treat them. I think that this interest gives a better understanding overall of diseases and disorders as how they are treated is often based on what is going on. This is helpful in diseases which do not only affect the brain.
As for how this class applied to future career plans, I have stated in previous blogs my desire to be a teacher. I am currently applying to graduate schools for pursue a Master’s in Education and wish to teach high school chemistry. Many of the disorders we talked about had some sort of relevance to teaching adolescents. Whether it is the knowledge of things like autism and concussions which have obvious relations or things like bipolar and depression which are often diagnosed in adolescent years.
Another thing that is an invisible take home message is the process which we used to evaluate and learn about each topic. Starting with a published research paper can be very scary. Even as a senior in college who has researched using countless published papers, it is still a daunting task to weed through all the ‘chemistry jargon’ and get to what the authors are trying to explain. Instead of being expected to understand the paper on our own we worked together to create a list of things from the paper which we did not understand or wanted more information about. I really liked this approach as it broke what often was an eight to fifteen page paper up into a simple list of things. The list was then researched further and presented to the class. To further understanding, we ended each topic with a class discussion. Discussion was great as it did not focus on just the chemistry but also on the ethics and real world applications of the different diseases and disorders.
This approach to learning is something I would like to use when I start to teach. I think it would be helpful to use relevant articles to supplement chemistry curriculum in high school and to introduce high school students to real world applications of the topics being discussed.
Overall, I am very glad that Neurochemistry could be my capstone. I really enjoyed the class not only for the topics discussed but also the freedom that the format of the class provided. This freedom made the class much more personal and made me feel as if I was not only a learner, but also a teacher.
1
This fall semester I decided to embark on an adventure through the mind by learning about different disorders and disease affecting our brain in the neurochemistry class at Concordia College. Prior to the first day of class, I thought the class was going to be very difficult and boring because of the overwhelming amount of biochemistry present in the subject. Also, I was concerned that I would be clueless about what was happening because I have had very limited exposure to diseases affecting the brain prior to this class. However, I was pleasantly surprised to learn that, although there is a lot of biochemistry, the class was one of the most satisfying classes I have taken at Concordia College and I recommend it to everyone.
What makes this such a great class? Well, I’m glad you asked. First, the class is set up differently than any other science class I have ever taken. Each week we attempt to tackle a new disease by investigating biological pathways which are disrupted as a result of the disease or disorder. Over the weekend we are assigned to read a research paper and write down questions that arise. In class on Monday’s background information about the paper is provided to help with our understanding of the disease or disorder. Additionally, questions are asked about the paper and these questions assigned to different members of the class to research and answer. On Wednesday, each member reports what they learned about their assigned question. Finally, during Friday’s class, the class is split up into groups and a discussion ensues about possible solutions to the disease or disorder. Honestly the Friday discussions are my favorite part because by the end of the week I feel I understand enough of the disorder and the research paper to adequately debate what is causing the disorder and if there is anything that can be done. Also I like our side-tracked discussions which tend to take place. After the discussion we write blogs about some aspect of what we learn through the course of the week and post it on the class blog page (the very site you are looking at).
Second, everyone can relate to at least to one or two of the disorders and diseases presented in the class. Although we did explore some conditions which few people in our class have been directly affected by, like bipolar disorder, most of the topics were familiar to everyone such as obesity, concussions, and alcohol consumption. This means people were more willing to research and debate the disorder or disease in class. So what I think makes this a great class is that I am encouraged to explore each topic as in-depth as I want and share what I have learned with others. I feel this is a more effective way of teaching than being told information and expected to memorize it for a test at the end of the class.
Finally, I would like to quickly say what I have learned as a result of taking this neurochemistry class. First, as I’m sure you have expected, I have learned a lot about the different types of diseases which we focused on in class. Prior to studying each disease I had little knowledge regarding of what the diseases were and how they worked in the body. However, now I view people with the disorders or diseases in a different way. Second, I feel more comfortable discussing hot button topics concerning the diseases and sharing information about the disease to others not in the class. Finally, I have learned how to present valuable information quickly and effectively as a result of our 3 minute time limit on Wednesday classes. This has helped me realize what information is important and which is not. Therefore, overall the neurochemistry course at Concordia College is an excellent way to learn of diseases and disorders seen daily in society and to see what is being done to help these people.
Source:
1) http://hplusmagazine.com/wp-content/uploads/brain1.jpg
1
Autism is a developmental disorder characterized by impaired social interactions and communication and is normally diagnosed between the years of 2-4. However, the number of people diagnosed with autism has been on the rise in recent years. In a news story released by MSNBC on May 29th 2012 1in 88 children are diagnosed with autism up from 1 in 110 in 2007.2 So what are the possible reasons for the increase in autism?
As part of our investigation into autism this week we discussed possible reasons why autism could be on the rise. One of the possible reasons we mentioned in class is that environmental factors, like consumption of heavy metals and xenobiotics, are causing oxidative stress in the brain and are disrupting biological pathways as a result. In the paper this week researchers suspect the xenobiotics, which are any chemical found in an organism but would not be found in the organism naturally, and heavy metals are causing oxidative stress which is interfering with an enzyme named methionine synthase. The methionine synthase enzyme is responsible for methylating DNA and dopamine-stimulated phospholipids. As a result of fewer methylations, neuron networks are having problems synchronizing with one another and therefore causing problems with attention and cognition. The most likely sources for these heavy metals and xenobiotics are from pharmaceutical medications, food, and possibly from pesticides and herbicides.
Another possible reason why autism has increased in recent years is that doctors have gotten better at diagnosing children with autism. Unfortunately there are no biological or blood test to help identify children with autism. Instead, children are diagnosed by doctors who look for problems with communication, social interaction, and restricted and repetitive behaviors. Additionally, parents are commonly questioned about the child’s behavior to see if it is unusual. As a result of the observations and help from the parents, the doctors are able to determine if the child does or does not have autism.
Finally, vaccines have commonly been associated with the rise in autism in United States. Although there is evidence that vaccines given to children do not lead to autism this idea still persists in the United States. The main ingredient commonly connected with autism is thimerosal which used to be a preservative in vaccines. However, evidence from studies examining trend in autism and vaccine use do not support a connection between thimerosal and autism.3
Although there are several hypothesizes as to what could possibly be causing the increase in autism the true cause is still unknown. Personally, I think, like with most diseases, there is not a single biological problem resulting in autism. Instead I think the rise in autism is due to better diagnostic techniques and an increase in the biological stimuli which are responsible for causing autism. What these stimuli are I am unsure. One thing is for sure, autism will continue to rise until we can determine what is causing the increase in autism cases.
Sources:
1)http://www.google.com/imgres?q=autism&um=1&hl=en&sa=N&tbo=d&rlz=1T4ADFA_enUS342US343&biw=1366&bih=630&tbm=isch&tbnid=UuEBVHHE5g7FfM:&imgrefurl=http://www.asasb.org/&docid=6GvuTf0ItKFOjM&imgurl=http://www.asasb.org/wp-content/uploads/2010/11/AutismAwarenessRibbon-162×300.jpg&w=162&h=300&ei=FgzFUKvbGuXa2wWLwYHgDg&zoom=1&iact=hc&vpx=496&vpy=146&dur=979&hovh=240&hovw=129&tx=67&ty=136&sig=117327967081406772799&page=1&tbnh=155&tbnw=83&start=0&ndsp=22&ved=1t:429,r:3,s:0,i:161
2) http://www.msnbc.msn.com/id/46892046/ns/health-childrens_health/t/better-diagnosis-screening-behind-rise-autism/#.UMJZbqP4LSk
3) http://www.iom.edu/Reports/2004/Immunization-Safety-Review-Vaccines-and-Autism.aspx













{kind=link}