What is Psychopathy?
Psychopathy is generally considered to be a more severe form of antisocial personality disorder (ASPD). Though it is important to note that there are differences between the two disorders. To start off, psychopathy is not an official diagnosis is the Diagnostic and Statistical Manual of Mental Disorders (DSM), which is used by the majority of mental health professionals to diagnose mental illnesses. ASPD is found in the DSM-5 and is considered to be an official diagnosis.
Both of these disorders display very similar symptoms which is why it is easy to get them confused. Psychopathy is marked by a lack of empathy, shallow emotions, impulsiveness, manipulative behavior, lack of remorse and guilt, and a disregard for social norms and the law.
While ASPD is marked by a disregard for and a violation of the rights of others, impulsiveness, aggression, lack of empathy, guilt, and remorse, irresponsibility, disregard for societal norms and laws, and substance abuse. Adults diagnosed with ASPD must also have been diagnosed with a different disorder called conduct disorder as a child or teenager. This is because the DSM doesn’t allow for children to be diagnosed with personality disorders, but ASPD generally begins to develop during a person’s mid-teenage years.
It is important to note that the most important difference between psychopathy and ASPD is that psychopathy is defined more by personality traits while ASPD is defined more by observable behaviors. However, neither of these disorders automatically makes a persona violent or a criminal.
How is the brain affected?
The direct cause of psychopathy and general antisocial behavior is still unknown, but there have been new discoveries on the genetic irregularities behind the disorder. Certain genes like PRL109 and ZNF132 have been found to be abnormally upregulated in people with psychopathy that have committed violent crimes. ZNF132 had the strongest association and is a gene linked to developmental and malignant disorders. It was found to have very high levels in the neurons found in the cerebellum. The cerebellum is not only in charge of fine motor movements but has also been found to regulate our social behaviors. The cerebellum does this by affecting the release of the neurotransmitter dopamine (DA) which is linked to our reward system. If there is too much of the gene ZNF132 in the cerebellum this causes the cerebellum to release incorrect of amounts of DA which could negatively affect social behaviors.
Another gene that was found to be important for the antisocial behaviors of psychopathy is the OPCML gene. This gene affects the opiate receptors in are brain. These receptors are important for regulating processes of pain, pleasure and reward. A dysregulation of the OPCML gene causes these receptors to not do their job effectively which adds to the explanation of antisocial behaviors. This gene can also help explain why people with psychopathy and ASPD are often also diagnosed with substance abuse disorders.
Finally, there has been a connection made between insulin resistance and antisocial behaviors. This insulin resistance is connected to abnormal glucose metabolism that is marked by the downregulation of the gene PSMD3. These abnormalities have been connected to impulsive and violent behaviors. This is possibly because the brain relies heavily on glucose and when it cannot metabolize glucose correctly this puts stress on the neurons and causes further dysregulation of functions throughout the brain, leading to antisocial and violent behaviors.
What can be done?
Unfortunately, there are not many treatments for psychopathy. This is partially because there is very limited research of the disorder. Currently to go-to for treating both psychopathy and ASPD is counseling or therapy. This counseling focuses on trying to teach people with psychopathy how to manage their behaviors and regulate their emotions. This treatment also focuses on teaching them how to recognize their behavior and interact effectively with others. For ASPD, some medications can be used to manage any severe anger or depressive symptoms.
But there is a new form of treatment emerging called the decompression model. This model of treatment has been tested on youths in Wisconsin that have been diagnosed with conduct disorder and have been arrested for criminal behavior. This model focuses on a positive reward system for good behavior rather than a punishment system for bad behavior. The aim of this treatment is to teach young adults with conduct disorder the benefits of following social norms so they will be less likely to resort back to criminal behavior. This treatment has shown impressive results, but more research still needs to be done to determine its efficacy for widespread use.
References
Fisher, K. A., & Hany, M. (2022, August 15). Antisocial Personality Disorder . National Center for Biotechnology Information. Retrieved April 4, 2023, from https://www.ncbi.nlm.nih.gov/home/.
Pomeroy, R. (2014, July 11). Can psychopaths be cured? . Real Clear Science. Retrieved April 4, 2023, from https://www.realclearscience.com/blog/2014/07/can_psychopaths_be_cured.html.
Promises Behavioral Health. (2023, March 1). Psychopathy vs. antisocial personality disorder. Promises Behavioral Health. Retrieved April 4, 2023, from https://www.promises.com/addiction-blog/psychopathy-vs-antisocial-personality-disorder/.
Tiihonen, J., Koskuvi, M., Lahteenvuo, M., Virtanen, P. L. J., Ojansuu, I., Vaurio, O., Gao, Y., Hyotylainen, I., Puttonen, K. A., Repo-Tiihonen, E., Paunio, T., Rautiainen, M. R., Tyni, S., Koistinaho, J., & Lehtonen, S. (2020). Neurobiological roots of psychopathy. Molecular Psychiatry, 25. 3432-3441. https://doi.org/10.1038/s41380-019-0488-z.
What is psychopathy? Psychopathy Is. (2023, February 24). Retrieved April 4, 2023, from https://psychopathyis.org/what-is-psychopathy/.
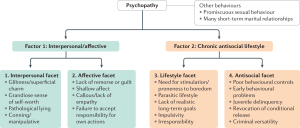 When diagnosing psychopathy, a questionnaire called the
When diagnosing psychopathy, a questionnaire called the 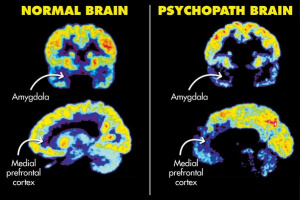 Researchers do not know much about the true cause of psychopathy and ASPD. Previous research has shown that there may be some
Researchers do not know much about the true cause of psychopathy and ASPD. Previous research has shown that there may be some  There are many stereotypes when it comes to the term psychopath. Most of these stereotypes come from media. Most notably, Joe Goldberg from the hit TV show You and Norman Bates from the hit TV show Bates Motel. The TV and movie industry has made a lot of money off of dramatizing people and the term psychopath, but these are not an accurate depiction of what it is like to live with the psychopath label (Norman and Norma Bates on the left and Joe Goldberg below).
There are many stereotypes when it comes to the term psychopath. Most of these stereotypes come from media. Most notably, Joe Goldberg from the hit TV show You and Norman Bates from the hit TV show Bates Motel. The TV and movie industry has made a lot of money off of dramatizing people and the term psychopath, but these are not an accurate depiction of what it is like to live with the psychopath label (Norman and Norma Bates on the left and Joe Goldberg below).
 Artstract #2
Artstract #2







:max_bytes(150000):strip_icc()/the-four-stages-of-sleep-2795920_FINAL-5c05c2fc46e0fb00018dac3d.png)

:max_bytes(150000):strip_icc()/how-to-get-better-sleep-5094084-regular-FINAL-2c371001cada4ad391f6de53fc6053c9.png)