
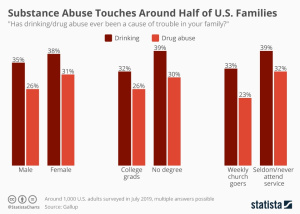
Addiction to drugs of abuse plagues all corners of America. From needles littering the streets of major urban centres to the hover of prescription opioid abuse in rural areas, it is a growing dilemma. Access to care is stretched and the problem is getting worse.. In fact, a release from the National Centre for Drug Abuse statistics reports that half of reporting individuals (aged 12 and up) have used illicit drugs at least once. There have been 700,000 deaths from opioid overdose alone since 2000. As this crisis has grown, solutions of varying degrees have arisen. Safe-drug use facilities have been proposed to help limit street drug use from an increasingly addicted population while others are working to stop distribution of drugs of abuse in its tracks. However, amongst proposed solutions, some of the fundamental causes of addiction can be forgotten. A review by Eric J. Nestler in Nature Neuroscience back in 2005 dives into what causes addiction at a cellular and molecular level.
The Dopamine System
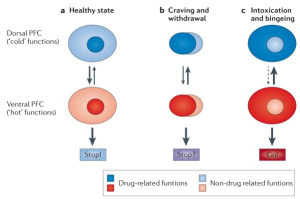
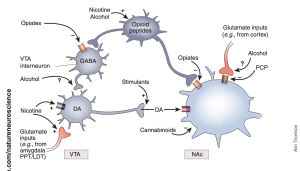
Otherwise referred to as the brain’s reward circuitry, the dopamine system plays a critical role in why drug addiction can develop. This system can be found in the ventral tegmental area of the midbrain and is also where the dopaminergic neurons within it target areas of the forebrain. A specific pathway is formed in this area called the VTA-NAc pathway. Drugs activate the transmission of the neurotransmitter dopamine within the pathway. When there is continuous activation of the circuit, tolerance to dopamine can occur while at the same time a sensitisation to the neurotransmitter develops. This occurs in combination with withdrawal symptoms that increase drug-seeking behaviour. Sudden withdrawal from use of a drug activates the central corticotropin releasing factor system; this will increase drug withdrawal symptoms. Drug use has also been linked to hypofrontality which is decreased function of the frontal lobe, which is responsible for complex thought processes. Hypofrontality can thus lead to less control over drug-seeking behaviour. With both dysfunction of normal reward signalling in the dopamine system, and increased drug withdrawal, addiction can ensue and magnify itself quickly.
Changes Occur Right Away
Another change occurs to the actual shape of neurons within this system. The neuron is much like a tree. The end of it that receives messages are projections called dendrites that are much like the leaves and branches that make a tree canopy. Drug use and addiction has been shown to affect the morphology of this “dendritic arbour.” Chronic cocaine, amphetamine, or nicotine exposure have shown increases in dendritic arborisation. This increase in the dendritic arbour contributes to drug sensitivity which furthers addiction in an individual. This process changes the actual shape of the neuron and helps demonstrate how persistent addiction can become. The figure below depicts the difference in size between the dendrites of addicted versus non-addicted individuals.
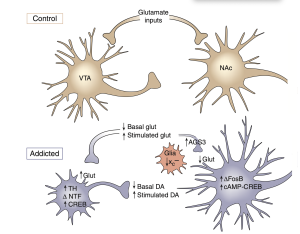
Figure 1. This is from Figure 2 of Nestler (2005) comparing the size difference between addicted and control dendrites.
What Should We Do?
With the addiction crisis we face, all cards need to be put on the table, but this review can help us understand two things that show addiction as a persistent disease rather than that of a mental toughness discussion. Drug addiction affects the brain’s sensitivity to dopamine making drug exposure have higher and quicker highs. It also leads to permanent morphological change to the neurons themselves affecting multiple parts of the brain’s reward pathway. Drug exposure can start the addiction process from the start and needs to be considered when exposing persons to drugs of abuse. The same also comes to the fact that environments contribute to someone’s susceptibility to drug reuse. Environments that systemically cue drug use amongst individuals will make fighting addiction a constant battle. However, armed with this knowledge, we can have empathy for those in their fight against addiction and continue to face this challenge in our future.
“Drug Abuse Statistics,” National Center For Drug Abuse Statistics, accessed 28 February 2023, https://drugabusestatistics.org
Eric J. Nestler, “Is there a common molecular pathway for addiction?” Nature Neuroscience 8, no. 11 (2005), 1445-1449
“Supervised Consumption Services,” Harm Reduction, accessed 28 February 2023, https://harmreduction.org/issues/supervised-consumption-services/



 Statistically,
Statistically, 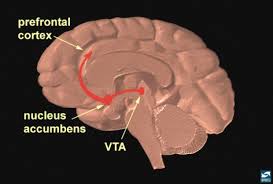 Addicts will choose this feeling over anything else in their life because eventually their brains don’t feel motivation or reward for any other activity other than using their drug of choice. Even with their drug of choice, they will eventually need to increase the amount they take to keep that high.
Addicts will choose this feeling over anything else in their life because eventually their brains don’t feel motivation or reward for any other activity other than using their drug of choice. Even with their drug of choice, they will eventually need to increase the amount they take to keep that high.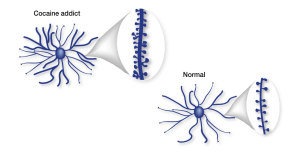 Part of the brain responsible for reason, judgment, learning, and memory begin to have changes as well. In some spots, the neurons are pruned back whereas in other regions there are more connections, completely changing the shape of the neuron. After all of these changes, the drug-seeking behavior becomes habit and the person becomes addicted.
Part of the brain responsible for reason, judgment, learning, and memory begin to have changes as well. In some spots, the neurons are pruned back whereas in other regions there are more connections, completely changing the shape of the neuron. After all of these changes, the drug-seeking behavior becomes habit and the person becomes addicted. Relapse is defined as when a person returns to using drugs or alcohol after a period of sobriety. There are many factors that contribute to relapsing, which can be seen in this image. After the neurons are changed and the feeling and memories of drugs are implanted into someones brain it can be extremely hard to just give it up. The brain is still searching for this increased reward feeling and it isn’t getting it from ‘normal’ daily activities which can make turning back to drugs really tempting.
Relapse is defined as when a person returns to using drugs or alcohol after a period of sobriety. There are many factors that contribute to relapsing, which can be seen in this image. After the neurons are changed and the feeling and memories of drugs are implanted into someones brain it can be extremely hard to just give it up. The brain is still searching for this increased reward feeling and it isn’t getting it from ‘normal’ daily activities which can make turning back to drugs really tempting.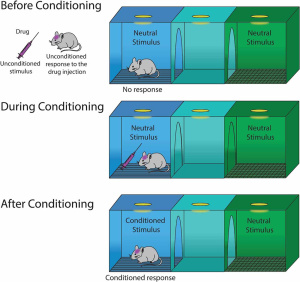 Conditioning is defined as a higher dose of drugs that can be tolerated when external stimuli is associated with prior administration of the drug is present. Basically, this means that if someone is doing drugs in the same room at the same time everyday they will eventually build up a tolerance because their brain will release the the effects of the drug before it is even taken. This leads to a tolerance, and if the drug is taken with any of the external factors changed it can lead to an overdose.
Conditioning is defined as a higher dose of drugs that can be tolerated when external stimuli is associated with prior administration of the drug is present. Basically, this means that if someone is doing drugs in the same room at the same time everyday they will eventually build up a tolerance because their brain will release the the effects of the drug before it is even taken. This leads to a tolerance, and if the drug is taken with any of the external factors changed it can lead to an overdose. Recovery is much more complex than it is made out to be. There are many factors that play a part in the life of an addict. It is not as simple as quitting cold turkey sometimes. There are memories and outside factors that can effect the ability to remain sober. Being educated on all the facts of addiction can help stop the stigma that it is just a simple choice. It truly goes down to the cellular and molecular level and changes are happening at those levels making it difficult to change behaviors right away. Treatment for addiction can be very expensive and difficult.
Recovery is much more complex than it is made out to be. There are many factors that play a part in the life of an addict. It is not as simple as quitting cold turkey sometimes. There are memories and outside factors that can effect the ability to remain sober. Being educated on all the facts of addiction can help stop the stigma that it is just a simple choice. It truly goes down to the cellular and molecular level and changes are happening at those levels making it difficult to change behaviors right away. Treatment for addiction can be very expensive and difficult. 




{kind=link}