
Since elementary school, I recall being told to get a “good night’s sleep” before tests – I, along with many other kids, did not take this seriously. In college, I finally discovered the importance of sleep, especially in organic chemistry when every night I was dreaming about SN2 and Grignard reaction mechanisms, waking up to a greater understanding and solidification of these concepts. Too often, I hear my fellow students talking about studying all night before exams as if it is going to help them – it does not! It is actually detrimental to their exam performance. Studies have found that fewer than 10% of college students sleep the recommended 7-8 hours at night during finals. How detrimental is this really? What does the lack of sleep really do? It has been shown that sleep, particularly REM sleep, is crucial for memory consolidation and long term memory formation.
Sleep
The sleep cycle is broken into NREM (non-rapid eye movement) and REM (rapid eye movement) sleep. NREM sleep consists of three stages in which the body repairs tissues and strengthens the immune system. REM sleep happens about 90 minutes after falling asleep and is important in the stimulation of the regions of the brain important for learning and protein production. REM sleep brain activity waves are comparable to waves seen during wakefulness and alertness. The stages of NREM and REM sleep are depicted below.

Hormones and Clock Proteins
Melatonin and cortisol are the primary circadian hormones and they are both produced in the pineal gland and released according to lightness or darkness. The retina at the back of the eye has photoreceptors called rods and cones that respond to light and darkness, and they have signaling attachments to the optic nerve which connects to the pineal gland. With darkness, melatonin is released and from the morning light, cortisol is released to wake us up. Melatonin increases the expression of the clock protein, PER1. This protein is of the period gene which encodes circadian rhythms of locomotion, metabolism, and behavior. Since melatonin increases this expression, it is concluded that PER1 plays the largest role in our decreased locomotion and metabolic rate in our sleep.
Memory Consolidation and Sleep
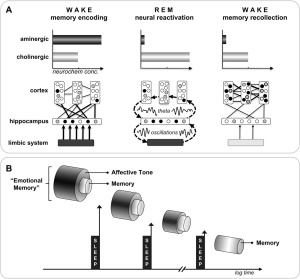
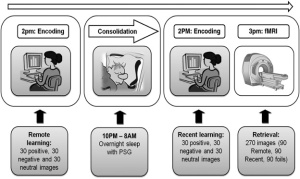
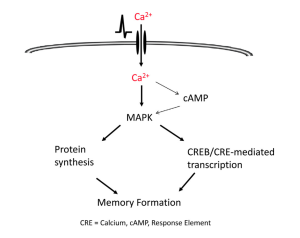
It has long been proposed that memories are consolidated in our sleep by, for example, dreaming of our awake experiences (like organic chemistry). However, the biological reasoning was lacking – until now! It has been found that the cAMP/MAPK/CRE-mediated transcription pathway, a key memory consolidation pathway, reaches a maximum during REM sleep. In individuals with dysfunction of this pathway, perhaps a sleep deprived individual, long term memory formation is blocked. In order for memories to be consolidated, there must be repeated reactivation of these signals to maintain required protein levels for persistence of these memories. This repetition actually occurs in our sleep! The suprachiasmatic nucleus is the “circadian pacemaker” of the brain, and it also controls the oscillation of cAMP, MAPK, and CREB levels. It has been found that this oscillation reaches maximum activity of these pathways during REM sleep!
In summary, during REM sleep a crucial memory consolidation and neuroplasticity pathway is at its highest activity, consolidating awake moments into long term memories. So, sleep the night before exams! If you study during the day, these concepts will replay during REM sleep and turn into a long term memory, maybe even making more sense when you wake up!
References
- Ryan, T. (2022). A Study Guide To Getting Sleep During Final Exams. Sleep Foundation. Retrieved March 22, 2023, from https://www.sleepfoundation.org/school-and-sleep/final-exams-and-sleep#:~:text=If%20school%20and%20sleep%20don,Fewer%20than%2010%25
- What are REM and Non-REM Sleep? WebMD. Retrieved March 22, 2023, from https://www.webmd.com/sleep-disorders/sleep-101
- Anderson, L. (2019). Melatonin and Cortisol. Thriven Functional Medicine Clinic. Retrieved March 22, 2023, from https://thrivenfunctionalmedicine.com/melatonin-and-cortisol/#:~:text=Melatonin%20works%20to%20keep%20circadian,which%20is%20our%20awake%20hormone.
- PER1 Gene – Gene Cards. Retrieved March 22, 2023, from https://www.genecards.org/cgi-bin/carddisp.pl?gene=PER1
- Xia, Z.; Storm, D. (2017). Role of circadian Rhythm and REM sleep for memory consolidation. Neuroscience Research 118, 13-20. https://doi.org/10.1016/j.neures.2017.04.011




:max_bytes(150000):strip_icc()/the-four-stages-of-sleep-2795920_FINAL-5c05c2fc46e0fb00018dac3d.png)

:max_bytes(150000):strip_icc()/how-to-get-better-sleep-5094084-regular-FINAL-2c371001cada4ad391f6de53fc6053c9.png)








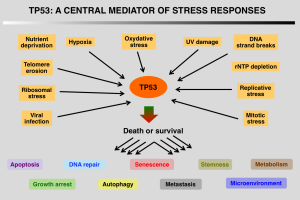 The transcription regulating characteristic of activated TP53 allows it to convert DNA to RNA, which will go on to create cellular responses to the stress that is happening. To link it to TP53s main ways of regulating cells, the RNA can code for DNA repair proteins, or proteins that will initiate apoptosis if the cell damage is irreparable.
The transcription regulating characteristic of activated TP53 allows it to convert DNA to RNA, which will go on to create cellular responses to the stress that is happening. To link it to TP53s main ways of regulating cells, the RNA can code for DNA repair proteins, or proteins that will initiate apoptosis if the cell damage is irreparable. TP53 is mutated or deleted from the genome in over 50% of all human tumors. When the TP53 gene is damaged tumor suppression is compromised, are people with this are likely to develop tumors in early adulthood. Well maybe increasing levels of TP53 can be a good solution to preventing tumors or the spread of tumors. While this has been researched, this can cause early aging in a person, which is something that not a lot of people are too keen about. However research has been done in aiding to restore functionality of already existing TP53 in order to treat cancer. In 2003 a gene therapy called
TP53 is mutated or deleted from the genome in over 50% of all human tumors. When the TP53 gene is damaged tumor suppression is compromised, are people with this are likely to develop tumors in early adulthood. Well maybe increasing levels of TP53 can be a good solution to preventing tumors or the spread of tumors. While this has been researched, this can cause early aging in a person, which is something that not a lot of people are too keen about. However research has been done in aiding to restore functionality of already existing TP53 in order to treat cancer. In 2003 a gene therapy called