We are all familiar with the term “the munchies,” but how does this happen?
Turns out, it has to do with the cannabinoid 1 receptors (CB1 receptors) and the effect on our appetite once there is binding with tetrahydrocannabinol (THC) to its active site. Once bound, our appetite is increased and hence the “munchies” effect.
But, where are these CB1 receptors even located?
It has been observed that there is an abundance in the cerebellum, basal ganglia, hippocampus, and dorsal primary afferent spinal cord regions of the brain. Basically, they are found all over the middle of the brain. They have also been present in some peripheral organs. For reference, here is a photo of what I meant by the middle:
There is a general lack of understanding surrounding the topic of marijuana and cannabinoids. Somethings most don’t know is the body naturally produces endocannabinoids that activate different CB (cannabinoid) receptors throughout the body. While it is true that the active ingredient in marijuana, THC, activates these receptors, there are many other ligands that do the same thing, most naturally produced in our body. There has been a recent surge in the use of medical marijuana and its derivations to treat complex medical disorders and diseases. CBD is growing increasingly popular for a plethora of different uses ranging in conditions from trivial to extreme. Taking a look at what we know and don’t is a great way to start an educated and engaging conversation around a lightning rod topic.
Endocannabinoids are signaling molecules in the body that help regulate various body processes. Among the eCB’s, the most common are AEA and 2-AG. These ligands are agonists for CB-1 and CB-2 receptors but bind CB-1 receptors with higher affinity. The role of cannabinoid receptors is increasingly under investigation as we find they’re interactions on several neural function is high. CB-1 receptors have an impact on many disorders in the CNS including many neurodegenerative disorders such as Huntington’s disease, multiple sclerosis, and Alzheimer’s.
While being different diseases HD, MS, and AD patients have all shown positive responses to treatment with CB-1 receptor agonists like THC or CBD.
https://mygolfspy.com/cbd-buyers-guide-golfers/
Aside: what is CBD? It seems to be talked about like a magical cure all by some. Does it make you high, and why can you buy it nearly everywhere? CBD, or cannabidiol, is one of the active chemicals in Marijuana, the second most active behind THC actually. While the binding affinity is not particularly high for either CB-1 or CB-2 receptors it does bind to certain serotonin receptors which explains its effect on anxiety, nausea, vomiting, and the perception of pain.
CB-1 receptors in particular are involved in many different functionalities of neurons and the CNS. In patients with Multiple Sclerosis, CB1 agonists are found to control inflammation. People who suffer from Huntington’s Disease often lose control of motor functions and these symptoms have been shown to mostly be alleviated by CB-1 agonists in limited studies. Similar positive responses have been seen in Alzheimer’s Disease, traumatic brain injuries, and other conditions involving a dysfunction in the CNS or peripheral neurons. However, research is pretty limited at the time as the field is very young.
Continued research is essential for expanding our knowledge of this complicated signaling pathway. There are cannabinoid influences in nearly all of our bodily functions. It is good to erase our preconceived notions on the term cannabis. There are proven results for treating complex diseases with cannabinoid receptor agonists. This doesn’t mean we should all be smoking marijuana as there are many other compounds involved and the research isn’t conclusive on their affects. However, research into THC, CBD, and other external cannabinoids is an important step in finding solutions to some of our most perplexing medical issues.
Obesity is an epidemic, not just in the united states but in a lot of countries in the world. It begs the question; why don’t people stop eating so much? The problem is the solution to this problem is more complex than a simple life decision. We all know the feeling of being hungry and full, what if there was a disruption in this signaling that is leading to obesity? Leptin is a hormone in the body that regulates the reserves of energy stored in adipose tissue, it works directly by acting in the brain to regulate appetite. One would think an obese person would have increased leptin signaling, and partially you would be correct, but the high concentrations of leptin have led to resistance in the neurons and an eternal feeling of hunger. Over nutrition then leads to a plethora of other problems, mainly caused by inflammation in the central nervous system and peripheral tissues. The pandemic has brought light to our lifestyles and how body image is portrayed in media culture.
artstract by Colin Richards
Before getting into the cultural anthropology of obesity it is important to understand the physiology. Rapid overconsumption of a fat-rich diet results in a two-phase inflammatory process in the hypothalamus. The first phase is a transient and the second comes from sustained exposure to a high fat diet, leading to prolonged inflammatory cascades and the activation of cellular stress mechanisms. Activation of transcription factors and the release of cytokines stimulate inflammation in the hypothalamus. The continuous release of leptin leads to resistance and adds fuels the problem. Without the necessary signaling of leptin a person is continuously hungry and continues to eat.
Body image has been a hot topic in media culture lately. Especially for women, but increasingly in men, there has been a criticism of unrealistic body expectations imposed by movies, models, magazines, etc.… There has been a calling to appreciate various body styles and sizes. This has brought light to multiple mental issues that revolve around people’s self-perception of their body. However, others have recognized the danger in this body appreciation as it celebrates an unhealthy lifestyle. Navigating this tightrope of mental and physical health is important for individuals and society. I believe it’s always important to be happy but knowing health is something we can all work on is equally important. Personally, I know being physically healthy positively affects mental health and I think changes in how we eat, and exercise will positively affect the mental health crisis we have.
Body image has been a hot topic in media culture lately, it coincides with a continuous growth in the obesity pandemic. Understanding the physiology of obesity is important when talking about the social issues around body image. Obesity is not an active decision and celebrating the body style supported by a consistent high fat diet is a slippery slope. The body changes in both the CNS and peripheral tissues from obesity are very detrimental to our health. The thin line between mental and physical health is where we should congregate.
This blog post is all about how neurochemistry class meets Concordia’s 5 goals for liberal learning and hones skills developed from other classes.
Install a love for learning
Reproduced from Pixabay
Neurochemistry achieved this goal through a few different avenues. I think the best example is the Friday discussions where we communicate with our classmates about what we learned. Not only did we discuss the relevant pathways and hypothesize novel treatments, but we also related it to topics that interested us. For example, we would discuss how insulin resistance contributes to Alzheimer’s disease mechanistically, and also what we can actively do ourselves to prevent the disease.
Develop foundational skills and transferable intellectual capacities
Wow did Neurochem develop this skill! Reading a research article every week greatly improved my skills as a researcher in many different fields. Additionally, the content we learned is applicable to many different fields including cancer biology, genetics, drug-design, and many more. Understanding the fundamental signaling pathways of life is a valuable skill for many different scientific disciplines.
Develop an understanding of disciplinary, interdisciplinary and intercultural perspectives and their connections
While neurochem was mostly sunshine-and rainbows, sometimes it took on heavy concepts like Alzheimer’s, obesity, autism, and drug addiction. There is a very clear connection between the signaling pathways we learned for these diseases to other scientific disciplines, but interestingly, there are clear connections to social work and public policy.
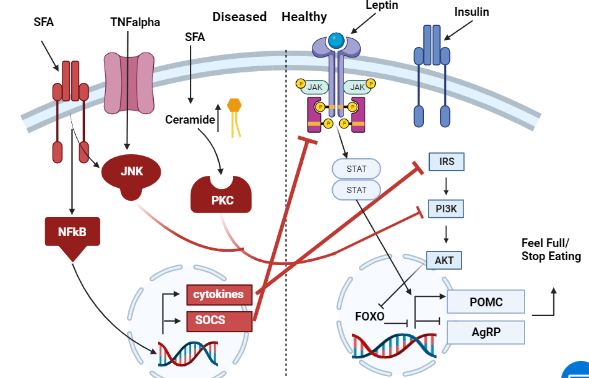
A very good example of this comes from the obesity paper we read. As you can see in the diagram (figure 1) below, SFA (saturated fatty acids–think butter) and insulin signaling play a role in regulating obesity.
Figure 1. Obesity Signaling. Made by Bretton Badenoch
While on the surface, these discoveries don’t seem to directly tie to socioeconomics and public policy, they assuredly do. A lot of the cheapest food consumed by the socioeconomically disadvantaged can cause insulin resistance and is often high in SFA. Furthermore, the connection between socioeconomic status (SES) and race is linked in the USA. Because of this, the implications of this knowledge apply across cultures and between disciplines both social and scientific.
Cultivate an examined cultural, ethical, physical and spiritual self-understanding
Boy oh boy did neurochem cultivate a whole lot of self-understanding. I think there are a few reasons people could be interested in studying neuroscience:
They are interested in others and want to understand how they work on a more fundamental level. The reasoning for wanting to understand can vary from nefarious to benevolent.
They are interested in themselves. They are curious about how they make sense of the world from a metacognitive level.
Personally, I’m in it for both reasons but I definitely lean towards #2 more. Because of this, I think neuroscience inherently forces one to examine their cultural, ethical, physical, and spiritual self. In many ways, neuroscience a very philosophical subject with immediate and implications for the student. For example, baring willful ignorance, it’s impossible to avoid examining the role free will (or the lack thereof) and its implications on nearly all social institutions.
Encourage responsible participation in the world
This is where we get super meta. The blogging aspect of this course IS the responsible participation in the world.
Reproduced from giphy
Rapid Fire Q and A
Q: What kinds of learning occurred during this semester?
A: Learning from published papers, peers, instructor, and other internet sources.
Q: How do the skills, competencies and knowledge gained in the experience (CAP, blogging) relate to your future goals?
A: I want to go to grad school for a PhD in biochemistry with a neuroscience focus, so this class was pretty perfect for me. Learning all of these fundamental pathways has helped me with research I am currently doing with designing new drugs to treat depression. It has also helped lay a solid foundation as a continue to learn more about neuroscience and neurochemistry in graduate school.
Q: What does learning at a liberal arts institution mean to you?
A: I think of an institution that promotes deep understanding of a certain topic, as well as supporting topics to make for a well educated person. A liberal arts institution develops a curriculum that allows for interdisciplinary connections between an intense area of study and the real world.
Q: If you were to highlight on your resume a skill or competency that you improved upon this semester, what would you be sure to include?
A: I would include the blog posts. I think dissemination of scientific knowledge in an accessible form is important for improving our democracy and the world we live in. I also feel like I really improved my graphic design skills this semester with the artstracts. I have notoriously bad handwriting and drawing/painting skills, so finding a medium I’m not awful in has been exciting.
Conclusion
This course developed the core competencies Concordia considers integral to its education through a variety of ways. Neurochemistry was a very engaging class with topics ranging from cool to mind blowing. My ability to read scientific papers was further refined in this course, as was my ability to draw conclusions form the papers. This class has already improved my research by giving me new ideas on what pathways need adjustment in a variety of illnesses. I think the knowledge gained in this class will carry with me throughout my education and future career.
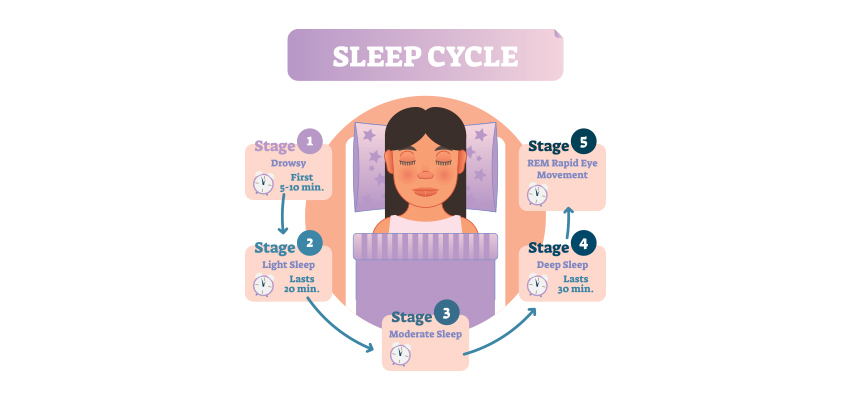
Stage 1 is when we first enter sleep and where our sleep is the lightest possible and can easily be disrupted. This is also when our muscles begin to weaken and our eye movement is slow.
Stage 2 is marked by slower brain waves. This is when our eyes stop moving. While brainwaves have begun to slow, there are brief periods of time where there will be short bursts of activity.
Stage 3 is classified as the period of entering deep sleep. Slower waves begin to show. During the 4th stage, the slower waves are at times interrupted with waves that are a little more hyperactive. during both of these stages is when an individual is in or has entered deep sleep. When individuals are awoken from these specific stages, they feel groggy and disoriented.
REM stands for “rapid eye movement” and that is exactly what occurs during this stage in sleep. Our eyes rapidly move back and forth while our breathing becomes more rapid and while we are paralyzed, our heart rate and blood pressure increase. An individual awakened from this stage can recall their dreams.
I found that this specified class was unique compared to the other ones that I have taken during my time at Concordia. However, it was a good experience that helped me be able to understand more on comprehending data and information on multiple scientific articles. From what I learned from this class, I believe that visual and audio learning, from reading, are important types of learning for me when trying to comprehend complex scientific writing. The visual imagery of each neural pathway helped me understand what exactly goes on in the brain, allowing myself to understand the scientific writing. Hearing myself talk and converse on the topic also helped me as well.
I found myself learning more on how to understand scientific writing styles and the skills, competences, and knowledge gained from this experience allowed me to apply this mode of study to other assignments and projects. An example in this instance is this senior seminar paper I am writing on solutions to climate change. The papers I read for my review are scientific articles and applying from what I learned on reading these types of articles in neurochemistry, I am able to comprehend what goes on in each of the experiments conducted in each paper. While this cannot be considered as a future goal right now, it was in November when I was writing my first draft for my review.
Along with applying this way of study to my assignments, it has helped me understand more on the concepts of vocational value and liberal arts. Learning at a liberal arts institution to me is learning how to create a strong sense of social responsibility and expand your vocational values, expanding your intellectual and practical skills, such as communication, analytical, and problem-solving abilities, and a demonstrated ability to apply knowledge and skills in real-world settings. These new skills that I have obtained can be highlighted on my resume as skills and competencies that prove that I have improved by way of thinking on a problem and answer it with the best answer possible. An example of a type of problem I solved was describing how two neural receptors are similar but have different functions when a mechanism is carried out. Reading carefully and efficiently through this part of the paper is key.
The skills I believe that I have improved very well are reading comprehension, statistical analysis, and visual learning through studying certain parts of each research paper, or article. This includes scientific functions of each neural pathway written in the paper, understanding the results of each experiment, and once again the ability to learn by seeing the example of the neural pathway present in the paper. Overall this type of class has shown me not just how to apply ways of study to a paper and understand it, but also to understand more on how each disease is caused and how certain mechanisms that happen in the brain develop. These were very interesting articles to read and I found that the course information was very interesting and fun to learn about.
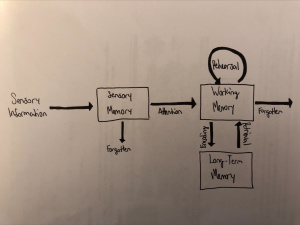
In 1900, the idea that memories require time to become resistant to disruption was proposed: the consolidation hypothesis. In order for sensory information to become a stable memory, there are three stages of memory in which this information must pass through:
Sensory Memory (SM) – very brief memory storage that holds impressions of recent sensory information
Holds information for 1 second or less
Working Memory (WM) – storage that allows an individual to recall and manipulate information for a short period of time
Holds information for 30 seconds or less
Long-Term Memory (LTM) – storage of various memories and experiences
Figure 1. Artstract depicting the memory stages and their relationship
The underlying mechanisms of memory consolidation include protein synthesis necessary for long-term potentiation (LTP). LTP is a process in which synapses between neurons are persistently strengthened through repeated activation that produces enduring signal transmission. LTP is a form of synaptic plasticity, which is simply a change at neuronal synapses (junctions). The synthesis of proteins is necessary for the construction of large, stable, actin cytoskeletons (spines) that promote endurance of LTP. In order to induce LTP and protein synthesis, Ca2+ influx through glutamate binding to NMDA receptor channels and voltage-gated Ca2+ channels is necessary. Also, intracellular stores of Ca2+ from the endoplasmic reticulum (ER) may be released through ryanodine receptors (RyR) or IP3R Ca2+ binding. Then, protein synthesis may either occur locally (within the dendritic spine), or may result from genomic cascades (synapse/soma to nucleus). Local protein translation begins when a dendritic spine become stimulated and increases translation of specific proteins used to synthesize proteins necessary for LTP. In order for this protein synthesis to occur, activation of signaling pathways such as MAPK or mTOR, each activated by the BDNF-TrkB pathway, is necessary (Rudy, 2008).
Impacts of Sleep on Memory Consolidation
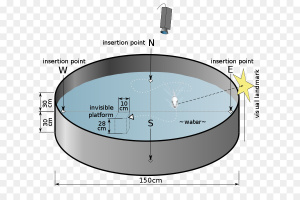
Figure 2. Morris water maze: learning and memory task for rodents
There are many studies that feature the benefits of sleep on memory consolidation. The neural connections necessary for memory stability have shown to be strengthened by sleep. While many researchers had initially stressed the importance of REM sleep for memory stability, many have shifted focus to non-REM (NREM), specifically slow-wave-sleep (SWS) (Cross et al., 2018). SWS has been shown to be heavily involved in the enhancement of declarative memories (facts and knowledge). Alternatively, REM sleep has been shown to improve consolidation of procedural memory (tasks). In animal models, deprivation of REM sleep following training in the Morris water maze (a rodent memory task) interfered with spatial learning and memory. It has also been shown that learning produces an increase in REM sleep. Interestingly, the onset and duration of REM sleep varies with task complexity (Xia and Storm, 2017).
Cellular Mechanisms
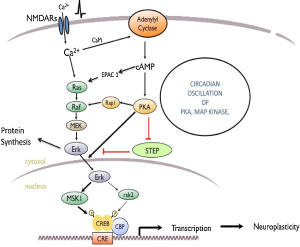
Although the underlying mechanisms of memory consolidation and sleep do not appear to be well-studied, certain researchers have begun to untangle some of its mystery. As stated earlier, Ca2+ release and activation of MAPK and mTOR signaling pathways is necessary for protein synthesis and the endurance of LTP. According to Xia and Storm (2017), Ca2+ influx through NMDA receptors activates CaM and the Ras/Raf/MEK/Erk signaling pathway (MAPK pathway).
Figure 3. The memory pathway (Xia and Storm, 2017).
The activation of CaM then activates adenylyl cyclase which promotes cAMP signaling to activate the MAPK signaling pathway as well. Upregulation of the MAPK signaling pathway positively regulates CRE-mediated transcription and protein synthesis necessary for LTP and subsequent memory formation. This signaling pathway maintains memory through circadian oscillations within the hippocampus during REM and SWS sleep, possibly reaching its maximum in REM sleep (Xia and Storm, 2017).
Sleep Deprivation (or Excessive Sleep)
Sleep deprivation has been shown to increase difficulty in memory retrieval and consolidation. It is likely that when one is sleep deprived (not getting enough REM or SWS sleep) the necessary signaling pathways are not being activated to promote protein synthesis and LTP. Also, many studies have hypothesized the idea of “overworked” neurons that are no longer able to function properly and retain necessary information. Due to this, it becomes much more difficult to access information learned previously. Conversely, similar symptoms may also be seen through excessive sleep. According to Ma et al. (2020), there is an inverted U-shape correlation between sleep duration and cognitive decline. This implies that too much or too little sleep can produce declines in cognitive ability, while intermediate sleep is necessary for optimal performance (Ma et al., 2020). Sleep recommendations for college students between the ages of 18 and 25 is 7-9 hours of sleep per night. In regard to learning and memory, sleep has been shown to be an essential biological process to promote health in the human brain and body.
References
Cross, Z. R., Kohler, M. J., Schlesewsky, M., Gaskell, M. G., & Bornkessel-Schlesewsky, I. (2018). Sleep-dependent memory consolidation and incremental sentence comprehension: Computational dependencies during language learning as revealed by neuronal oscillations. Frontiers in Human Neuroscience, 12. https://doi.org/10.3389/fnhum.2018.00018
Ma, Y., Liang, L., Zheng, F., Shi, L., Zhong, B., & Xie, W. (2020). Association between sleep duration and cognitive decline. JAMA Network Open, 3(9). https://doi.org/10.1001/jamanetworkopen.2020.13573
Rudy, J. W. (2008). The Neurobiology of Learning and Memory. Sinauer Assoc.
What kinds of learning occurred for you during this semester?
Fall 2021 held many opportunities for learning—both in the academic sense and the personal sense. I learned all sorts of neurochemical pathways in class this semester, and many of them will stick with me for a long time. I have already shown off my knowledge about neurochemical pathways to my parents, and I will continue doing so for the rest of my life. Most of my learning this semester, however, took place in the personal sense. I learned what type of learner I am (yes, it took four years to figure this out). I learned that I am a visual learner, as writing out a pathway helped me really understand it and extrapolate on it. I also learned where I am most confident in terms of topics.
What does learning at a liberal arts institution mean to you?
Learning at a liberal arts college means that I learn the skills I need to be a well-rounded individual. Learning at a liberal arts institution means that I learn the skills I need to be successful in my field, but I also learn the skills that I need to become responsibly engaged in the world. I tried to come up with a better phrase for it, but Concordia hit the nail on the head with that phrase. Learning at a liberal arts college means that you explore disciplines that are different from yours and, by doing that, you are able to bring the skills you learned from one class into the other. For example, I am a science major, but I had to take a few courses in the humanities area of study. I chose to take a class called Culture, Identity, and Dialogue. Going into the class, I was prepared to be bored out of my mind. My favorite subject to learn was science, and this class was the complete opposite of science. However, the global studies course ended up being one of my favorites that I have ever taken at Concordia. This class was completely different than one I have ever taken, and it challenged me to think differently about the world around me. Learning at a liberal arts college means that you challenge yourself to take on new perspectives through the lens of different disciplines and investigate how you might be able to use those perspectives in your specific field of study. Learning at a liberal arts college is all about exploring other perspectives and integrating them into other fields of study.
If you were to highlight on your resume a skill or competency that you improved upon this semester, what would you be sure to include?
If I were to highlight particular skills on my resume that I improved upon in this semester, I would highlight team-work. I would make it a fancier term on my resume, but I would highlight this skill for sure. In this course, we worked together on a project where half of the people had a different background than we did. I honed my skill of being able to work with others in a setting where the team members have different knowledge and different skills. I also would highlight the “clear communicator” skill. Some of this skill was improved upon through my job, but this course also taught me a lot about how to communicate complex topics to people who are not at the same understanding as I am. I learned how to describe complex processes in simple terms (most often in the form of metaphors). I also learned how to communicate my thoughts more effectively with someone who has a similar background to me. I am often intimidated by other’s knowledge, but I learned how to accept that I won’t know everything and just communicate what I do know.
Final Thoughts?
I grew a lot this semester—both in my academic and my personal life. These two pieces of me also influenced each other, which led to even more learning. I discovered my inner self-confidence, and I learned how to put myself first. I learned that being imperfect is okay, and I learned to not underestimate myself. I know and understand more than I think I do, and sometimes it just takes a little bit of work for me to see that. This class (along with physical chemistry) taught me a lot about the world. I learned that there is always more learning to be done, and I learned to think critically about issues within the field. But I also learned more about myself through these courses. I am truly grateful for all of the things I have learned through this course and throughout the semester.
Before you begin to read the rest of this post, I ask that you watch this video.
Fig. 1. An image of the little boy in the video mentioned above. Retrieved from : https://knowyourmeme.com/memes/have-you-ever-had-a-dream-like-this
What you just watched is one of my favorite videos on the internet. Whenever I see this video on a platform, I watch the whole thing and just smile the whole time. In case you didn’t feel like watching the video, I will also describe it. The video is just twenty seconds long and consists of a little boy attempting to ask the audience if they were had a dream similar to one of his. However, the audience is unable to recall a similar dream, due to the child’s inability actually ask the question. He tries to ask but cannot form a complete sentence until the very end of the video and, even then, the question still doesn’t make sense. I had you watch this video for two reasons: 1) I was hoping to put a smile on your face and make your day a little bit better and 2) I wanted to pose a similar (?) question to my audience (you).
What is the most memorable dream you’ve ever had? I’ve had many memorable dreams, but there is one set of recurring dreams I had that I will probably remember forever. I call them recurring because, though the actual plot of the dreams had nothing to do with the other, the ending was always the same. The first one took place at a river near my childhood home, one which had a strong current. The second dream took place in the ocean on the boat from Suite Life on Deck (shout out if you remember that show). TRIGGER WARNING. In both dreams, my brother’s death was the end of the story. In both dreams, he died due to drowning. I had these dreams probably in middle school, but I still remember them like I dreamt about them last night. You’ve probably had equally impactful dreams—ones that make you forget you’re dreaming, ones that you could retell with astounding accuracy. Now, researchers aren’t exactly sure why we dream when we sleep, but many dream theories have to do with memory consolidation.
(Also, just so you don’t think I’m a psychopath for dreaming about my brother’s death, he had a dream where I was mauled by a pack of wild dogs, so we are even).
Sleep and Memory Consolidation
Memory consolidation in the hippocampus follows a pretty distinct pathway, starting with the NMDA receptor. The NMDA receptors are most commonly known for their role in learning and memory, so it is no surprise that these receptors are the starting point for memory consolidation. Once the NMDA receptor is activated by glutamate, this triggers a cellular influx of calcium. The influx of calcium into the cell activates adenylyl cyclase, which then increases the production of cAMP. The increased production of cAMP activates PKA, which then activates Ras and the rest of the MAPK pathway (Raf, MEK, and ERK). Then, MSK-1 is activated, which phosphorylates CREB and triggers the transcription and translation of the CRE gene. To break it into chunks, and maybe help with the understanding, the first part of the pathway is G-protein signaling. The middle piece of the pathway is the usual MAPK pathway, followed by activation of a transcription factor. The figure below outlines this pathway.
Fig. 2. An image of the memory consolidation pathway in the hippocampus. Retrieved from: http://dx.doi.org/10.1016/j.neures.2017.04.011
Now, you may be wondering how the memory consolidation pathway in the hippocampus relates to sleep. This is a very good question, and I will answer it for you. The memory consolidation pathway is active during REM sleep. In addition, many of pieces of the CRE transcriptional pathway are modulated by the PER1 protein. The PER1 protein is an essential protein in the circadian cycle, and this protein oscillates cAMP, Ras, MAPK, and CREB. The circadian cycle refers to the physical, mental, and behavioral changes that follow a 24-hour cycle. Circadian cycles are primarily stimulated by light input thus, it controls the sleep-wake cycle. During the circadian cycle, an individual’s proteins are expressed in various levels depending on what point in the cycle an individual is on, which is referred to the circadian oscillations of the protein. So, PER1, which is an essential clock protein, controls the circadian oscillations of cAMP, Ras, MAPK, and CREB. Thus, in REM sleep, PER1 is responsible for the strength of the expression of these proteins after the pathway has been activated.
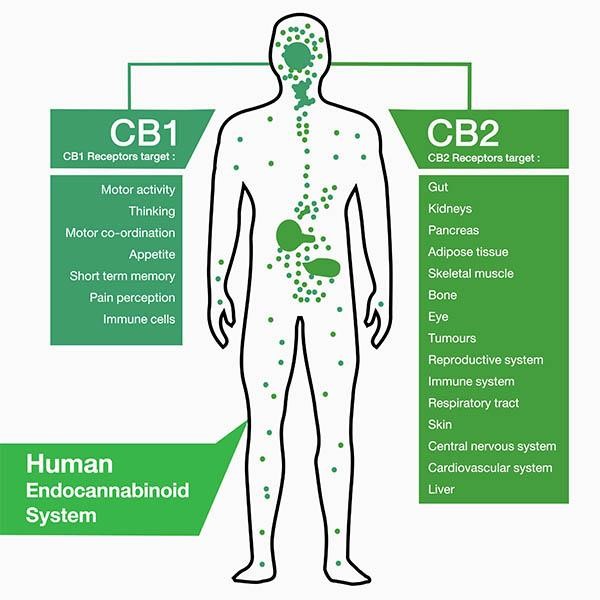
The systems in the body are very well known in protecting it, with the immune system protecting against infection and the integumentary system protecting against debris. However, the endocannabinoid system is not a very well known system within the human body. This is a surprise as it has proven to have multiple helpful functions. It is described to play a key role during synaptic plasticity and homeostatic processes in the brain, making it a suitable spot for therapeutic treatments for disorders of the central nervous system [1]. It is involved in the use of Cannabis for your body as a therapeutic and treatment.
The endocannabinoid system is composed of two main receptors. The two main receptors of the endocannabinoid system are the CB-1 and CB-2 receptors, which determine the behavioral effects of the body when cannabis is consumed [2]. The CB-1 receptors are mainly located in the brain and other nerves throughout the body while the CB-2 receptors are mainly located in the immune and gastrointestinal systems [2]. The way these receptors work is that the CB1 is activated by arachnidonylethanolamine and 2-arachidnonylglycerol, coupling the CB-1 receptor to G proteins leading to the inhibition of adenylate cyclase activity leading to a decrease in levels of cAMP [1]. Locations and Targets for both receptors are shown on the diagram below.
The Cb1 receptors tend to bind to the central intoxicating component of cannabis, tetrahydrocannabinol , making the Cb1 receptor play a major role in the euphoric effects of marijuana [3]. This means that when activating Cb1 receptors in your body this means that you have possibly smoked marijuana. Some of these symptoms that a person may experience in this situation includes the feeling of being on a high, pain relief, appetite, sedation and motor impairment, and cognitive and memory impairment [3].
The Cb2 receptors show another approach for brain disorder treatment by controlling synaptic functions involved in drug abuse and synaptic plasticity by inhibiting dopaminergic firing from the ventral tegmental area and reduced cocaine self-administration [1]. Based on the information gathered on both receptors, it is evident that the Cb1 receptor and Cb2 receptors are working around each other when exposed to cannabis.
While the endocannabinoid system has been linked to having roles in neurological diseases, there is some evidence of the receptors involved in treating people infected by the SARS-CoV-2 virus. Hypotensive effects have been shown to be caused by activation of Cannabinoid receptor 1 (CB1) and mediation by ACE inhibition [4]. These effects have been linked to direct vasorelaxation effects that were induced by CB1 activation or ANG (II) vasoactive agonists [4]. Along with CB1 receptors, CB2 receptors are known to exert anti-inflammatory and immunomodulatine effects when stimulated [4]. This is present in the human lungs making it possible to use CB2 as a target for treating SARS-CoV-2 infections by reducing inflammatory responses.
This information shows that while the use of marijuana can have severe side effects on people who use it to the highest extent, there is a possibility that it can be used for treatment purposes through activation of the Cb1 and Cb2 receptors leading to the reduction of COVID-19 symptoms and infections. This is why it can be very useful to learn more on how the endocannabinoid system can have possible therapeutic and treatment effects on the person’s body.