Figure 1: The chemical structure of propranolol.
The use of propranolol
The most commonly prescribed medications typically tend to be those that target immediate health issues such as pain or heart problems. Propranolol is one such medication that is common prescribed for hypertension, coronary artery disease and tachyarrhythmias. However, this medication can readily enter through the blood brain barrier, so there uses can be much more then simply an heart medication.

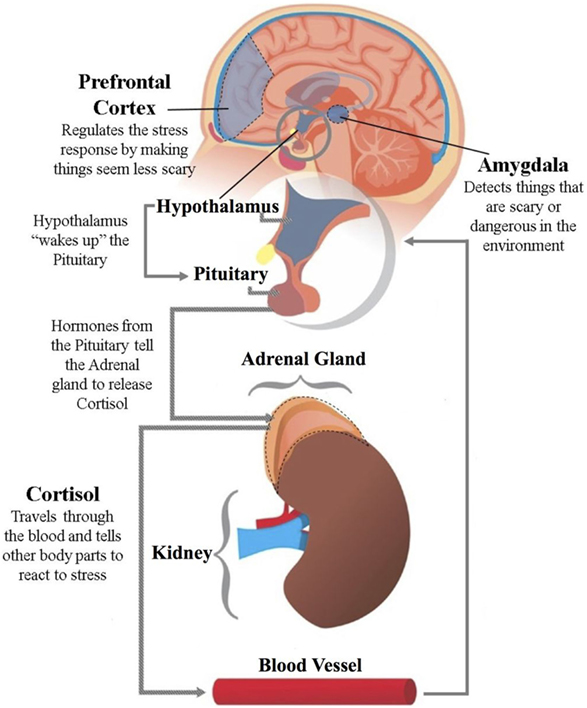
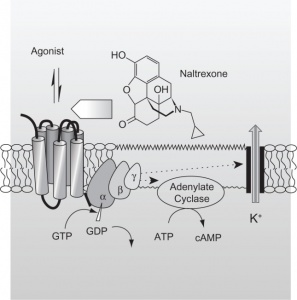
Figure 2: Diagram of the blood brain barrier.
Mechanism of action
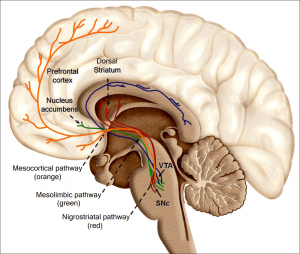
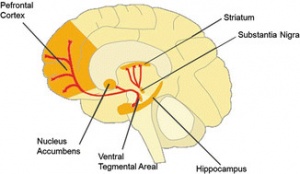
As seen in Figure 2 above, the blood brain barrier can be pretty tricky to cross. So, those medications that can offer a cascade of treatment possibilities. In the case of propranolol, it is a β 1,2-adrenoreceptor antagonist which will compete at the receptor level with catecholamines, thus blocking their effect. This mechanism has also been deployed to block β1,2-adrenoreceptors in the central nervous system. So, it is through the blocking of the catecholamines (adrenaline, noradrenaline, and dopamine) from binding to their corresponding adrenoreceptors that propranolol is able to reduce anxiety.

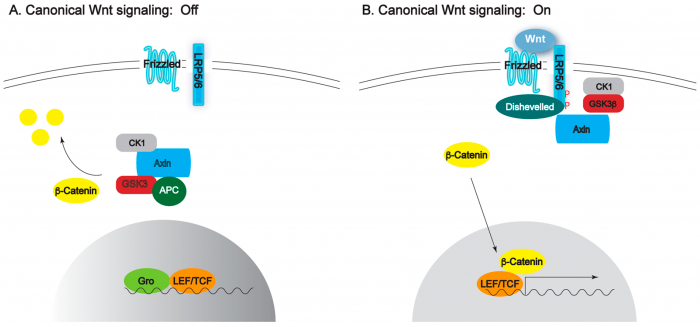
Figure 3: Commonly used SSRIs used in treatment of anxiety and depression
Why isn’t propranolol prescribed for anxiety?
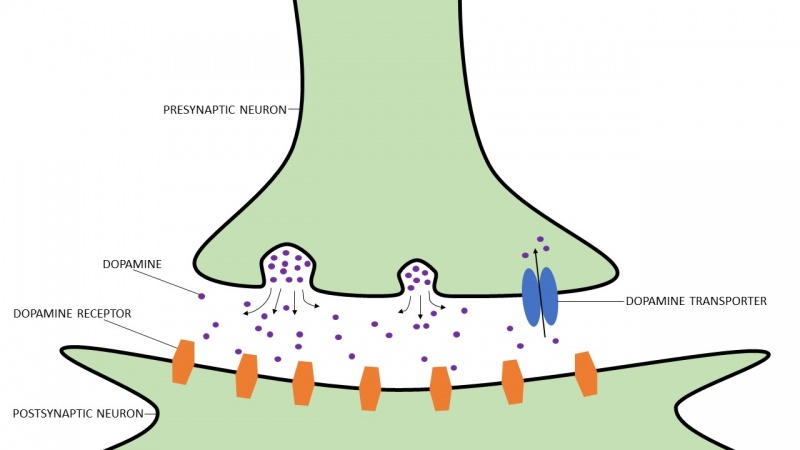
While the use of propranolol offers many promising results in both animal models and its use in humans, the world of treatment went a different route in the treatment of anxiety. The more recent prevalence of selective serotonin reuptake inhibitors (SSRIs) took the scene before propranolol could be effectively implemented for the treatment of anxiety. SSRIs, as the name implies, act to block the reuptake of serotonin in the synaptic cleft after it has been released. The presence of serotonin in the synaptic cleft has been proven to be an effective treatment for an assortment of disorders, but I’m mainly focusing on anxiety. So, it isn’t so much that propranolol isn’t used because it isn’t effective, but rather because there are more popular substitutes instead.

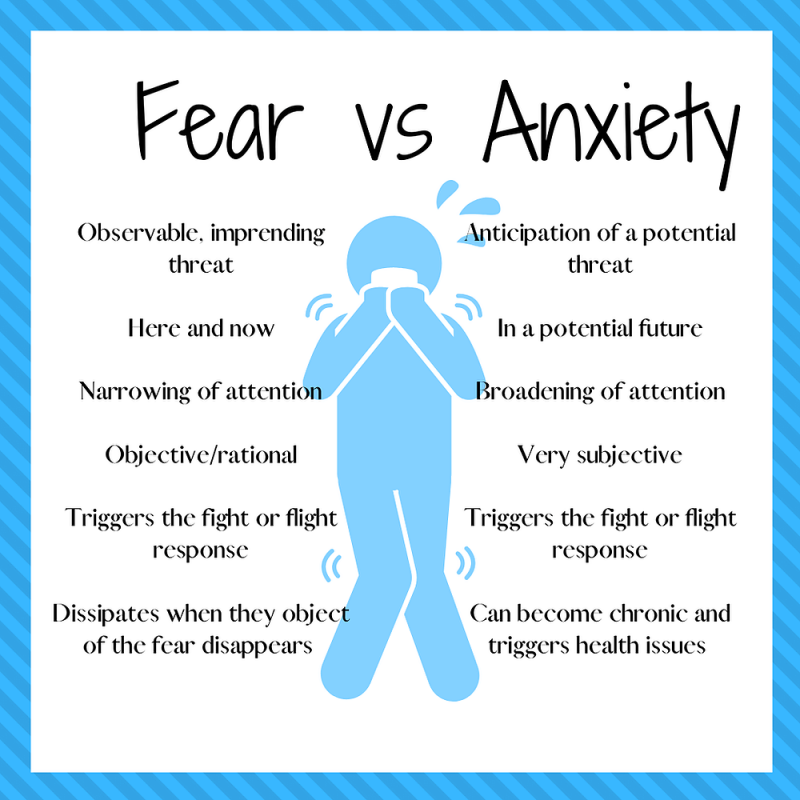
Figure 4: Generalized pathway for how stimuli is converted into long-term memories.
Function relating to memory
For the article we discussed in class, we mostly looked at how anxiety and stressful situations contribute to memory. This was seen with the use of the forced swim test as the stressful situation led to an increase in memory of the test as well as a corresponding change in behavior (reduced time to begin the immobile phase of the forced swim test). To continue with the idea of anxiety and memory, propranolol actually has an effect on this too!
As seen in Figure 4 above, there is a consolidation step that occurs after short-term memory that helps to convert sensory stimuli into long-term storage. This typically involves protein synthesis. Propranolol acts by selectively inhibiting this protein synthesis of fear inducing stimuli so that the fear memory is unable to be reconsolidated and converted into a long-term memory. It is believed that the selectivity acts by inhibing the feeling of fear in the memory, but leaving the overall memory of the stimulus otherwise unchanged.
The use of propranolol
As discussed above, propranolol is a commonly prescribed heart medication that also has to ability to help treat anxiety disorders, quite effectively. However, because of SSRIs shared ability to cross the blood brain barrier and the increased popularity of SSRIs, propranolol has been reduced to being prescribed for heart problems. But who knows, maybe in those that do have it prescribed, it is doing wonders!
For more information about propranolol, please see the following article here.
Also included is an artstract. I have a couple friends with diagnosed anxiety disorders and when I asked them what it felt like, they said they just get so overwhelmed by nothing and everything at the same time. So , I tried to get that in my drawing.

:max_bytes(150000):strip_icc()/ptsd-treatment-2797659_FINAL-5c12be374cedfd00010f866a.png) (4)
(4)