Music and the Brain
If you think about it, we hardly go anywhere that does not have some type of music playing in the background; the grocery store, driving in the car, the gym, and the list goes on. We are so often encompassed with music that we may not even know that is playing. Most people would probably just assume that a store or company is just playing the music to have some sort of background noise while a person goes about their business, but without even knowing, the music being played might be affecting something even stronger than our passive thoughts: our brains. Although a fairly new science, the impact of music on the brain is indeed an exciting one.
Where and what?

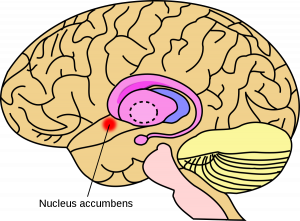
Studies using function magnetic resonance imaging (fMRI) have shown that when music is played, various regions of the brain respond. The frontal lobe responds and strengthens signaling to music due to the due to its purpose in decision making and planning. Since the temporal lobe processes what we hear, it is also triggered when listening to music. Also, music can be seen as sort of an addictive drug due to the fact it enhances signaling in the nucleus accumbens which releases dopamine in the reward system. These are just a few to describe, but music can also affect areas like the occipital lobe, Broca’s area, the cerebellum, the amygdala, the hippocampus, the hypothalamus, and even a few more. Since listening or playing music affects so many areas of the brain, it would make sense that a variety of reactions are triggered that affect our behaviors and feelings. Music has the ability to help a person recall a memory that might be associated with the song, can reduce stress, and music can even goes as far to be used to help patients who have acute or chronic pain, have had a stroke, or who have epilepsy. To understand music’s full capabilities, more extensive research will be needed, but it is definitely exciting to think about the possibilities!
Managing pain with music
Those dealing with chronic pain, like patients with fibromyalgia, or those dealing with acute pain, like pre- or post-operative patients, may benefit from introducing music therapy as an additive treatment to their pain treatment. It may seem like an abstract concept now, but recent studies have began to show how music can help those in pain and may be able to

reduce the amount of opioids or other pain killers prescribed. One study showed that dopamine release peaked “immediately before peak emotional response.” This response is also correlated to endogenous opioid signaling. When a person experiences a “wanting” emotion towards hearing a pleasurable song there is an increase in the circulation of endogenous opioids and an increase in the presence of the mu opioid receptor. With this understanding, scientists and researchers have theorized that music could potentially be a complementary treating to pharmaceuticals in treating pain. This means that the dosage or need for opioids could possibly be decreased immensely which could in turn reduce opioid addiction prevalence. The scientists who conducted the study mentioned above, found that using a technique called automated discovery showed the most pain reduction. This technique uses an algorithm to compile playlists that are tailored to a person’s music interests but continues to provide new music to its listener. Patients with chronic pain were “treated” with this type of music therapy and ended up showing a decreased need for opioid treatments for their pain. Although there is still much more research needed to completely understand the role of music on the brain, the potentials for music therapy seem endless and extremely beneficial for many health aspects.




 The collaborative format of these discussions from days one through three erased my concerns of being the least knowledgeable in the class as we all brought our own expertise and passion into the topic at hand. I was able to relate ideas about Alzheimer’s, spirituality, ecology, animal behavior, and dozens more topics based on other classes I’ve taken and on personal experiences. I ‘blossomed’ in this course as I felt emboldened to ask questions and share ideas I had, confident that I was adding to the discussion rather than making myself look silly.
The collaborative format of these discussions from days one through three erased my concerns of being the least knowledgeable in the class as we all brought our own expertise and passion into the topic at hand. I was able to relate ideas about Alzheimer’s, spirituality, ecology, animal behavior, and dozens more topics based on other classes I’ve taken and on personal experiences. I ‘blossomed’ in this course as I felt emboldened to ask questions and share ideas I had, confident that I was adding to the discussion rather than making myself look silly.