After spending the past fifteen weeks reading and discussing articles, creating a community outreach project, learning more about the brain, and deepening relationships with my friends, I find that I’m really sad for it to be over. So, if you’re a Concordia Student on the fence about taking this course, here are my top seven reasons why you should take this class.
- Read & discuss cutting-edge academic articles. For students pursuing a career in science, the ability to read and understand scientific papers is critical. In Neurochemistry, you hone this ability every week by reading a recent, comprehensive review paper on a given subject. Through this, my ability to read, understand, and critique scientific papers grew so much. As a future researcher, this skill will be one I’ll use constantly throughout my career.
- Course organization. Another key piece of what makes Neurochemistry unique is how the course is designed. Each unit is one week in length, with Monday holding a discussion of that week’s article where you have the chance to ask questions and seek clarification, Wednesday for ‘speed dating’ where you have 2 minutes to explain a topic people had questions about on Monday to the class, and Friday where you have a student-led discussion of topics relating to the paper. This layout removed the pressure of feeling like you had to completely understand the article for class on Monday and helped me deeply engage with the topic at hand.
- No lab. While I love being in a lab and doing experiments, I found that I really enjoyed not having an accompanying lab for this class. This feature of the course allowed me to focus on understanding a broad range of topics and dive deeply into each topic each week. Additionally, since labs are often 4-8 hours per week, not having an accompanying lab time made ironing out my schedule for this semester much easier.
- Deepen relationships with your cohort. People are so important. I cannot express how thankful I am for the people in my neuroscience cohort. Due to the discussion-based nature of the class, I got to know students in my major that I wasn’t close with before. Not only are the students in this class some of the most highly motivated individuals I’ve had the privilege to know. They’re also some of the kindest people as well. I’m excited to carry these professional and personal relationships into my future career.
- Learn from the experiences of others. Since neuroscience is an intensely interdisciplinary major, students often also double major or minor in other disciplines like biology, chemistry, psychology, religion, and environmental studies. Due to my heavy biology & chemistry coursework, I hadn’t had the chance to develop strong relationships with students with more experience in psychology, environmental studies, and social work, until now. Their contributions helped broaden my perspectives and added important context to our class discussions.
- PEAK-ing during Neurochemistry. While I think it likely that no adult would like to think of themselves as ‘peaking’ during college, yet I proudly did. At Concordia, PEAKs, or Pivotal Experiences in Applied Knowledge, are an opportunity to take the knowledge gained in the classroom and apply it to the broader world around us. In Neurochemistry, PEAK students are partnered with students in the Social Work department to create a community action project applying neurochemistry to benefit the community around us. My PEAK group examined the literature surrounding adverse childhood events, trauma-informed educational practices, and the neurobiology of PTSD and decided to create a video for education majors on understanding and identifying PTSD in children. Due to COVID, we recorded the video using Zoom and sent the video to the education club on campus, creating a resource that can be accessed by future students on demand.
- Finally, this class is really, really fun. Most of the time, it didn’t even feel like a class, but more of a journal club or book club with my friends. After all, what could be more fun than talking and learning about science with your friends?
Conclusion
So, are you convinced that you should take Neurochemistry? Well, even if you weren’t convinced by this brief blog, it’s a required course for the Neuroscience major and an elective for the Chemistry major so it’s likely that taking it might even be required for you. Additionally, it’s a great way to get one of your two required PEAK requirements for graduation! If that’s the case, hopefully, this blog piques your interest.



 that medication such as opioids do. This in part is why music has been shown to be capable of triggering short-term behavioral changes while also temporarily inhibiting feelings such as stress and/or anxiety. In fact, music that is non-lyrical with a low pitch and/or slow tempo (types that I personal enjoy listening to while studying) have been shown to be most effective at reducing stress and anxiety!
that medication such as opioids do. This in part is why music has been shown to be capable of triggering short-term behavioral changes while also temporarily inhibiting feelings such as stress and/or anxiety. In fact, music that is non-lyrical with a low pitch and/or slow tempo (types that I personal enjoy listening to while studying) have been shown to be most effective at reducing stress and anxiety! Of course, there will be a select number of individuals who have more benefits through listening, but this is what covers the majority of individuals. There are two factors that this largely comes down to. The first being that playing an instrument is normally far more of an active process than is listening to music. Your fingers and hands are usually both doing different things at the same time while your eyes dart across the sheet music. Most of the time when music is on, the only “active” thing we do is sing along and that can be thought of as more of a pleasurable aspect versus “testing” your brain to see how accurate you can be on wording and pitch. Researchers have been quoted as saying how this process “
Of course, there will be a select number of individuals who have more benefits through listening, but this is what covers the majority of individuals. There are two factors that this largely comes down to. The first being that playing an instrument is normally far more of an active process than is listening to music. Your fingers and hands are usually both doing different things at the same time while your eyes dart across the sheet music. Most of the time when music is on, the only “active” thing we do is sing along and that can be thought of as more of a pleasurable aspect versus “testing” your brain to see how accurate you can be on wording and pitch. Researchers have been quoted as saying how this process “










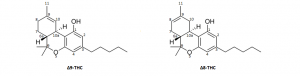
 Legalizing marijuana has been a pressing debate throughout the past decade. Our generation has been able to be front and center on this hot topic. Slowly, we are witnessing states legalize it both medically and recreationally. The legalization allows for many benefits along with consequences. In a recent class discussion, we were able to discuss the endocannabinoid system (ECS) and the possibility of using marijuana-based products to activate this system. Activation of ECS is useful because the system
Legalizing marijuana has been a pressing debate throughout the past decade. Our generation has been able to be front and center on this hot topic. Slowly, we are witnessing states legalize it both medically and recreationally. The legalization allows for many benefits along with consequences. In a recent class discussion, we were able to discuss the endocannabinoid system (ECS) and the possibility of using marijuana-based products to activate this system. Activation of ECS is useful because the system