The first thing many people think of when someone starts talking about cannabinoid signaling likely isn’t how cannabinoid exposure can change how your brain processes signals by directly modulating the number of receptors on neurons but likely has something to do with how recreational marijuana has been talked about in media or in pop culture. While there’s certainly nothing wrong with thinking of marijuana’s recreational uses first, cannabinoids do so much more for the human brain than create the ‘high’ associated with recreational marijuana use. Cannabinoids, a wide family of molecules, have been used to treat pain, muscle aches, anxiety, and even reduce the risks of addiction development when used in place of opiate pain medications. However, I’m most fascinated by how they directly change the number of receptors present on individual axons, leading to the formation of drug tolerance.
This is where beta-arrestin comes in. Let’s dive inside the brain.
Inside the brain: How beta-arrestin alters receptor concentration on post-synaptic neurons

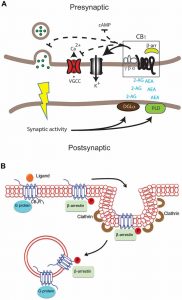
Figure 1. Graphic showing GPCR activation and eventual endocytosis via beta-arrestin signaling. (Ma L, Pei G. 2007. β-arrestin signaling and regulation of transcription. Journal of Cell Science. doi:10.1242/jcs.03338.)
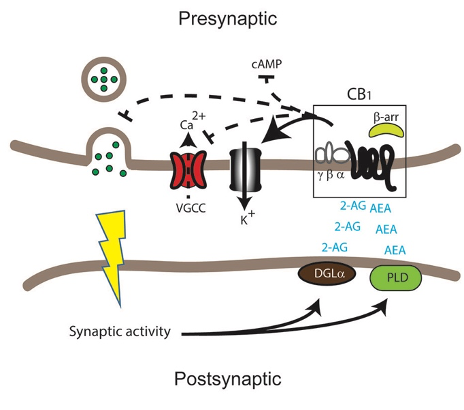
Let’s break it down. First, a ligand (a small signaling molecule) will bind to the GPCR on the extracellular (outside) part of the neuron. This is what tells the GPCR to activate. Once the ligand binds, the g protein dissociates from the GPCR and its alpha subunit, an effector protein, goes off to trigger the response. After the alpha subunit leaves the GPCR, GRK2 binds to the beta-gamma subunits of the GPCR and removes them, phosphorylating the GPCR’s tail in the process. This leaves the phosphorylated tail open for beta-arrestin to bind to it. Once beta-arrestin binds to the tail of the GPCR, it triggers endocytosis, bringing the entire GPCR into the cell in a small bubble of the cell membrane. This leads to desensitization by reducing the number of receptors available to respond to a given signal.
“That’s great,” you might say, “I now understand beta arrestin’s impacts on GPCRs, but how do endocannabinoids activate beta-arrestin?”
Great question. I’m glad you asked it. Let’s talk about it.
It’s actually pretty simple. Repeated exposure to cannabinoids that function as ligands for CB1 receptors increases GRK2 activity, thereby also increasing both beta-arrestin signaling, and GPCR endocytosis. This helps explain why some individuals who use cannabinoids repeatedly build up a tolerance, requiring more of the cannabinoid to achieve the same feeling. For example, THC, the cannabinoid found in recreational marijuana responsible for the “high” associated with its use, is likely the most well-known example of this effect.
Conclusion
In closing, there are two things I think you should take from this.
- Endocannabinoid signaling can be complicated. Beta arrestin’s role in changing receptor concentrations was only discovered in the last 20 years and its stimulation by endocannabinoids is still being understood.
- There’s still so much that science does not understand about how the brain works. It’s both a daunting and highly exciting prospect.

 We’ve looked more deeply into how the endocannabinoid system works in our body, but it’s also important to highlight the
We’ve looked more deeply into how the endocannabinoid system works in our body, but it’s also important to highlight the 
 explored to further depth
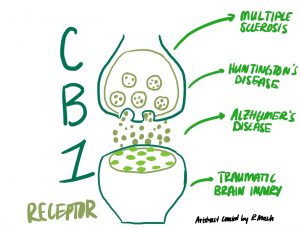
explored to further depth  that are influenced by the eCBs, with just a few listed below:
that are influenced by the eCBs, with just a few listed below: genetically or pharmacologically. The
genetically or pharmacologically. The 


 disturbances, etc.), this appears to not be great for our overall health. These disturbances typically lead to a low grade, local inflammation of the gut, which then turns systemic. Because of the gut-brain connection, systemic inflammation becomes neuroinflammation, or inflammation of the brain’s tissue. This can have all kinds of adverse effects that can show themselves behaviorally, or change the way the brain functions. Since the gut can affect the brain negatively like this, there are also positives that can occur. One of the major upsides that research is looking into is that we may be able to address and treat issues that are commonly associated with the brain, such as anxiety and depression, through the gut.
disturbances, etc.), this appears to not be great for our overall health. These disturbances typically lead to a low grade, local inflammation of the gut, which then turns systemic. Because of the gut-brain connection, systemic inflammation becomes neuroinflammation, or inflammation of the brain’s tissue. This can have all kinds of adverse effects that can show themselves behaviorally, or change the way the brain functions. Since the gut can affect the brain negatively like this, there are also positives that can occur. One of the major upsides that research is looking into is that we may be able to address and treat issues that are commonly associated with the brain, such as anxiety and depression, through the gut. to neurodegenerative diseases such as Alzheimer’s disease or Parkinson’s. Basically, inflammation is really not great, and can cause a cascade of negative effects that can happen over a period of decades. The good news though, is that inflammation can be treated using endocannabinoids, but that also doesn’t mean we shouldn’t try to prevent inflammation in the first place.
to neurodegenerative diseases such as Alzheimer’s disease or Parkinson’s. Basically, inflammation is really not great, and can cause a cascade of negative effects that can happen over a period of decades. The good news though, is that inflammation can be treated using endocannabinoids, but that also doesn’t mean we shouldn’t try to prevent inflammation in the first place. 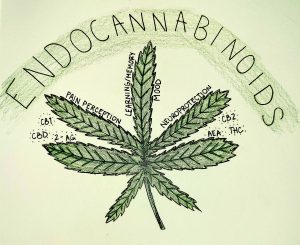

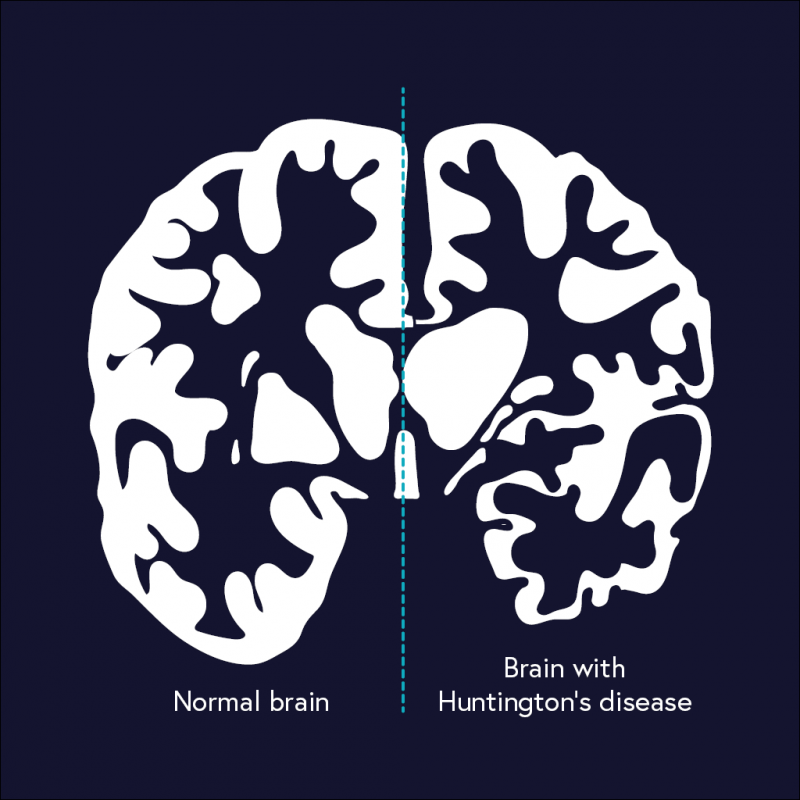
 Because the endocannabinoid system assists with memory, reduction of inflammation, and protection from neurodegeneration, it makes sense that dysregulation of the system could play a role in Alzheimer’s Disease. Evidence also supports a role of the system: levels of key molecules are off in AD brains and CB1 and CB2 receptors are correlated with tau tangles and other hallmarks of AD.
Because the endocannabinoid system assists with memory, reduction of inflammation, and protection from neurodegeneration, it makes sense that dysregulation of the system could play a role in Alzheimer’s Disease. Evidence also supports a role of the system: levels of key molecules are off in AD brains and CB1 and CB2 receptors are correlated with tau tangles and other hallmarks of AD.