Imagine going through your life as a healthy kid, both physically and mentally, and then one day everything changes. You start to hear voices from people who are not visually present – you start to hallucinate – and you develop an intense distrust of people you have interacted with and had relationships with for years. Schizophrenia does not look like this for everyone and not everyone has a sudden onset of symptoms, but these occurrences are very common with many people living with schizophrenia.
A Journey to Being Diagnosed with Schizophrenia
Tanara was diagnosed with Schizophrenia at 27, but the years leading up to that diagnosis were not easy. Five years prior to her diagnosis, Tanara developed symptoms of paranoia, hallucinations, and hearing voices. These symptoms persisted, and the next year she was hospitalized, followed by being given series of medications. Her symptoms stopped, and she thought everything was back to normal. This cycle of symptoms, medication, and a seemingly resolved mood disorder happened again over the next two years or so. Then, a breaking point led to her diagnosis with Schizophrenia.
Tanara lost her grandmother and suffered a hysterical breakdown, followed by being jailed over a fight with a neighbor. She was ordered to go to a psychiatric hospital where she was diagnosed with schizophrenia. From then on, she began a medication regimen and therapy to learn about and cope with her symptoms, and from there she began to take back control over her life.
Now, Tanara has a job where she is thriving, and she is more hopeful than ever about her future. Being able to recognize her triggers and knowing that schizophrenia doesn’t define her is crucial for her continued success. (To read Tamara’s full story, click here.)
Misconceptions about Schizophrenia
“People with schizophrenia are always dangerous.”
Reality: It is rare for people with schizophrenia to be violent. Actually, people with schizophrenia are more often victims of violence than the ones committing violent crimes.
“People with schizophrenia need to be in a hospital.”
Reality: Modern treatment methods are a combination of (but not limited to) medication prescriptions, out-patient therapy, and various lengths of hospitalization.
“Bad parenting causes schizophrenia.”
Reality: There is no evidence that parenting methods have an effect on the chances of developing schizophrenia. Genetics, however, do come into play in the chances of developing schizophrenia.
“Schizophrenics have multiple personalities.”
Reality: While a confusion of reality and fantasy may happen, multiple personalities are not part of the schizophrenia diagnosis.
You can read more about the misconceptions about schizophrenia here.
The Science Behind Schizophrenia
The exact processes of Schizophrenia are unknown, but momentous steps have been taken in determining exactly what causes this disorder and how the disorder actually affects the chemistry of the brain.
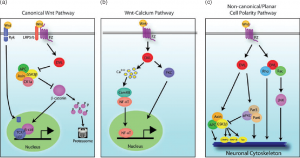
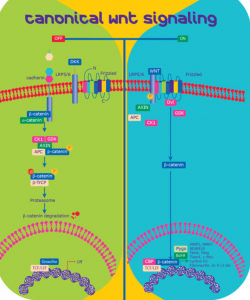
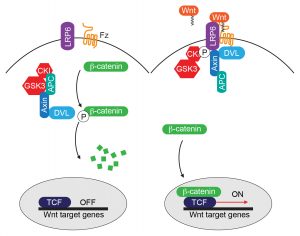
The various wnt pathways are depicted. Click here to read more about these schematics.
One pathway that is implicated to have a major role in understanding schizophrenia is the Wnt signaling pathway. The Wnt signaling pathway is dependent on a Wnt ligand binding to its receptor so to promote the proteins APC and Disheveled to gather and dissociate the glycogen synthase kinase 3 b (GSK3b), which is a destruction complex targeted at keeping b-catenin phosphorylated. b-catenin maintaining its phosphorylated state leads to the decease in concentration of cytosolic b-catenin, which ultimately affects the initiation of T-cell factor/lymphoid enhancing factor (TCF/LEF)-mediated gene transcription.
When we think of making everlasting memories, we often think of “the good” – road trips with friends, victories at athletic contests, adventuresome family vacations. If you’ve had such experiences, then recollecting these memories is likely to bring a smile to your face. But what happens when “the bad” becomes unforgettable? What happens when traumatic events or negative experiences become so ingrained in memory that day-to-day living becomes difficult? This is the reality for nearly 8 million adults every year, who suffer from a mental illness called post traumatic stress disorder (known as PTSD). There is no way to predict when trauma will happen, and for this reason there are no reliable ways to prevent the disease. Likewise, there are currently no end-all cures or treatments for this debilitating disorder, and the reason why some people develop PTSD and others don’t is still a scientific mystery. Nonetheless, recent research has shown some light on the ominous world of PTSD. In a world where people are exposed to war, crimes, and a variety of not-so-great experiences, finding new ways to help, support, and treat victims must begin with the basics – understanding the science behind what is unforgettable.
PTSD – A Mental Battlefield
One of the most relevant examples of PTSD in today’s world is the story of the returning soldier. The soldier returns after war overseas, reunites with family, and lives happily and safely at home for the rest of his life, right? Unfortunately, we are all too familiar with the reality that follows. Instead of living happily ever after, the soldier is startled at the sound of a shutting door, grows anxious from the revving of a car engine, or is shocked by the explosive nature of fireworks on the Fourth of July. Though not present in all soldiers, PTSD has been found to impact a notable portion of veterans, police, and first responders (all careers which can put someone in stressful situations). In essence, PTSD is a mental disorder that is triggered by either witnessing or experiencing an extremely stressful or traumatic event, such as warfare. Symptoms and implications vary in intensity, but among some of the most notable are:
Severe anxiety
Flashbacks, or reliving the event
Unwanted memories of event
Nightmares or dreams
Avoidance of situations or discussions that might serve as reminders
Some degree of depression, detachment, or feeling numb
Insomnia
Irritability
Hypervigilance, being easily startled or frightened by “normal” events, sounds, images, etc (also called “stimulus generalization”)
Though PTSD patients often share similar symptoms as those with other stress and anxiety disorders, PTSD has recently been identified as its own “category” of mental disorders. For a full list of symptoms, risk factors, and advice on working with PTSD patients, visit, you can visit the Mayo Clinic webpage here.
Sufferers of PTSD often experience relationship problems and self-destructive behavior that interferes with daily life. It is often hard for victims to think about anything else, let alone anything positive. At this point, stress becomes pathological. Despite its severe implications, little is known in terms of how this stress disorder manifests itself in the human brain. What do the scientists think? Keep reading to find out!
When Memory Becomes Pathology
It’s very easy to get lost in the weeds of behavioral and psychological aspects of PTSD, but like every other mental illness, PTSD must start with a change in the brain. A quick read of this recent review paper offers potential explanations for a variety of factors that might contribute to such changes. The subjects can be quite confusing, and it can be hard to imagine how each piece fits into the big picture. It helps to keep one main question in mind when trying to describe such complicated processes:
What happens in the brain after a stressful event that turns a memory into pathologic symptoms?
We will begin by attempting to answer this question. Specifically, how does the brain change in response to stress, and why do such changes cause PTSD in some victims of trauma? To oversimplify things a bit, it boils down to mainly two things: epigenetics and gene expression.
Gene expression refers to the process of converting DNA code into things (such as proteins and amino acids) our cells need to live, function, and carry out their specific tasks. Expressing different genes can lead to different outcomes or products.
Epigenetics refers to changes or modifications in a cell that can alter gene expression, without changing the original DNA code itself.
How does this relate to PTSD? Research suggests that stressful events cause epigenetic changes inside neurons (brain cells) that alter gene expression and thus their function – and ultimately the brain’s function. There are multiple elements that work together to cause this change. A simplified proposed pathway of these elements is detailed below:
Looks complicated, doesn’t it? Let’s break it down step by step.
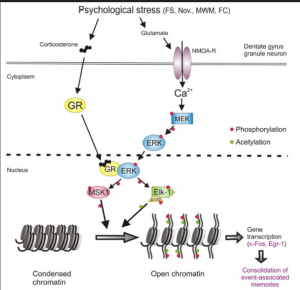
Stress and Stress Hormones: The word that every adult can relate to. Stress often comes with negative associations, and in the case of PTSD it’s no different. In the brain, stressful events (especially acute, traumatic events) trigger the release of stress hormones. These hormones are called corticosteroids and glucocorticoids. In addition, an increase in the amount of an excitatory neurotransmitter called glutamate is observed. This neurotransmitter tends to excite neurons, which is part of the reason why we are often awake and alert during stress! These increases are seen especially in parts of the brain necessary for emotion, memory, and fear – the limbic system. Notable parts include:
Amygdala (fear, aggression, emotional learning)
Hippocampus (memory consolidation and formation)
Dentate Gyrus (part of the hippocampus, used when forming distinct memories)
Epigenetic Change: This step can be easiest understood by looking at a forced swim rat study. The test does essentially what it sounds like – it forces a rat to swim for a period of time. It serves as a means of eliciting a “traumatic” or stressful memory in a rat and seeing how the rat behaves afterwards. Essentially what happens is:
Rat placed in water, forced to swim
Rat grows stressed and frantically swims
After a while, the rat goes still (called the immobility response, or learned helplessness)
Rat is removed from water
Just keep swimming, just keep swimming…
If the rat remembers this traumatic experience, then it will grow immobile in a shorter amount of time if placed in another forced swim test, having remembered what happened in the previous test. Interestingly, scientists found that an epigenetic change is responsible for the formation of this memory, and the development of the immobility response. Using a method called chromatin immunoprecipitation, or CHIP (not the edible kind), scientists were able to look at changes in chromatin (genetic material within cells) following a stressful event. The chemical change that literally “marked” the formation of this strong memory was found in a protein, called a histone (conveniently named H3s10KM), in the dentate gyrus. Here’s the chemical rundown:
Stress hormones bind to stress hormone receptors in brain cells, creating complexes
Meanwhile, glutamate interacts with its own receptors, called AMPA and NMDA receptors, normally important for long term memory formation. More basic information about this can be found here
Calcium moves into the cell through NMDA. This leads to chemical changes that activate a series of enzymes (called MEK and ERK, specifically – scientists are really good at giving names!)
ERK interacts with stress hormone receptor complexes
This interaction leads to a phosphate “on switch” being added to (you guessed it) more enzymes. The one we are interested in here is called Elk.
After being exposed to a particular electric signal from a brain cell (called p300, in response to the stressor), Elk adds a chemical group called an acetyl to the histone.
Adding an acetyl to this histone “opens” the cell’s DNA at some particular genes (formally known as immediate early genes), which makes it easier for them to be reached and expressed. These genes have been found to regulate stress responses.
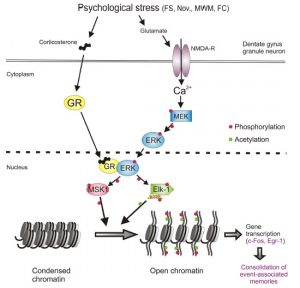
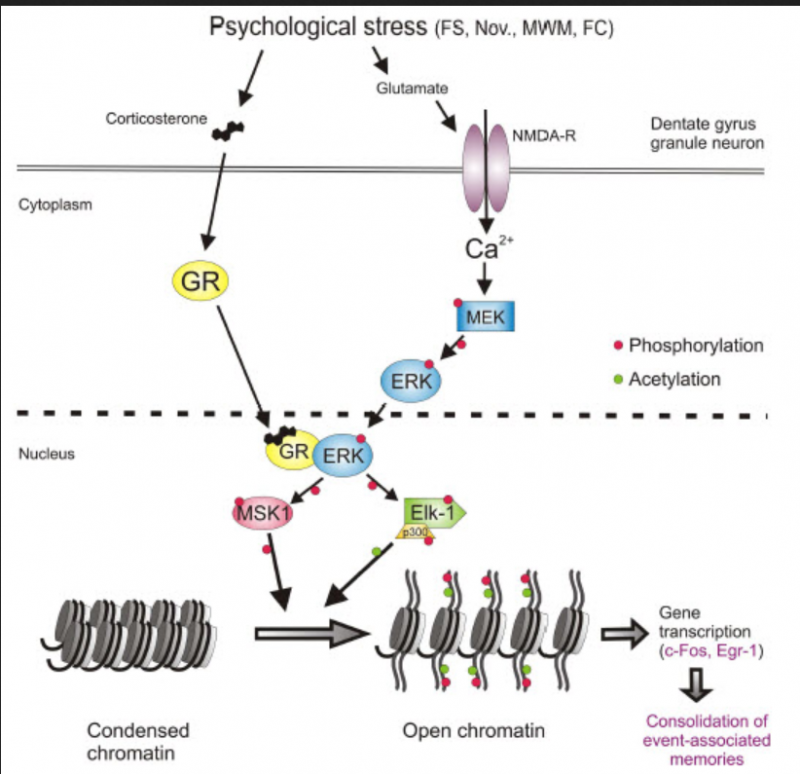
Interestingly, using chemicals that block the development of this acetyl “mark” or made the patheay malfunction led to rats that panicked every time they were placed in a similar situation, similar to what is observed in PTSD patients. If you’re more of a visual learner, here’s a helpful figure from the text:
Changes in Glutamate Transmission and Brain Damage: Seems like quite the process doesn’t it?If you haven’t stressed yourself out reading about epigenetics yet, here’s what happens next. The particular function of these “exposed” genes isn’t exactly known, but it’s predicted that they can change glutamate release throughout the limbic system, and this might lead to higher levels of glutamate in these parts. If you read the article linked above, you’ll know that glutamate is normally considered “the good stuff” – it helps with learning via interaction with AMPA and NMDA receptors and getting neurons all fired up! Normally, glutamate helps learning by activating a process that recruits more AMPA receptors to neurons (in a region called a synapse, these are what we think of when we hear “neuron connections, but it’s actually an empty space!). These receptors make it easier for neurons to respond to incoming signals. This explains why rehearsing something over and over makes it easier to remember – your neurons respond more easily to an incoming stimulus! But like the mantra goes, too much of a good thing isn’t great. So what happens if there’s too much glutamate? In a nutshell:
Neurons may become overexcited
Too much glutamate accumulates and becomes toxic
Can promote epigenetic change, which messes with the gene expression mentioned above, enhancing the cycle and stress responses
Hyperactive recruitment of AMPA receptors may strengthen memory of the stressful event
Too much stimulation in the limbic system can lead to anxiety, insomnia
An overactive amygdala can “overwork” the hippocampus (which tries to “calm it down”), leading to damage in this area of the brain
Damage to the dentate gyrus leads to loss of ability to distinguish distinct memories from each other, which can lead to fear and anxiety from what we’d consider “normal” events
Symptoms of PTSD manifest
The bottom line: like most things in life, glutamate is best in moderation. At such dramatic levels, which can result from being exposed to a traumatic event, the making of a memory truly becomes a potentially harmful pathology.
Victory for Victims – Treatments for PTSD and the Future
Although we are far from finding an efficient, effective pharmacologic treatment for PTSD, the paper above details some existing research done on animal models to study behavior that stems from learning and memory. Studying the behavior of rats in response to administering specific drugs that target the mechanisms described previously offers us a look at what works and what doesn’t. Currently, drugs often used to treat other mental disorders can be used to treat the symptoms of PTSD. These include
Antidepressants
Anti-epilectic medication
Anti-anxiety medications
NMDA antagonists (only tested in the lab, and not safe for healthy individuals)
Sadly, there aren’t many approved medications for treating PTSD, due to the sheer number of undesirable side effects. The most successful modern treatment for PTSD is not chemical – it’s largely based on behavioral therapy. Research on animal models has even found that something as simple as exercise can lessen symptoms of this disorder! But having PTSD also doesn’t spell out the end. Many PTSD patients are able to improve their symptoms to some extent, and some even make significant steps towards full recovery. When brainstorming modes of prevention though, there is one big question that looms overhead…
How stressful does an experience have to BE to trigger PTSD?
The true answer is we don’t know – and we might never. Why do only some victims of trauma develop PTSD? We don’t know. Memory formation is an extremely complicated topic in itself, and how we respond to and perceive our memories varies from person to person, rat to rat. How the brain decides what is stressful enough to literally “leave a mark” and what is so insignificant we won’t even notice is beyond our understanding. The brain in itself, like PTSD, is a mysterious object in science. Nonetheless, how we act depends on what we remember.
When it comes to common illnesses in the US, diabetes and Alzhiemer’s disease are often quick to make the list. Alzhiemer’s is a type of brain disorder that afflicts an estimated 5.8 million Americans each year, and type 2 diabetes is a metabolic disease that affects a whopping 27-28 million people living within the States. Despite these figures, however, many would be surprised to learn that these seemingly separate diseases share a surprising link. Alzhiemer’s associated with an increased risk of developing type 2 diabetes (and vice versa). Not only that, but in recent years, scientists have found that a hormone whose role is often only heard of in diabetes – the infamous insulin – plays a major part in the brain as well. So how exactly are these pathologies that affect different parts of the body related, and can Alzhiemer’s produce symptoms that could essentially be labeled as another type of diabetes? Keep reading to find out!
Sadly, we all know the story about a grandpa who can’t remember his son’s name, or a grandma who keeps forgetting where she put the keys. Alzheimer’s, or AD for short, is a neurodegenerative disorder (one that damages the nervous system) that leads to memory loss and inability to form new memories. Currently, the condition cannot be reversed or slowed by any existing medicine. Other symptoms might include:
Repeating statements
Forgetting scheduled events
Trouble talking, seemingly lost in speech
Getting lost, even at home
Misplacing items consistently
For a full list of symptoms and what you can do for someone experiencing AD, you can visit the Mayo Clinic page, (here)
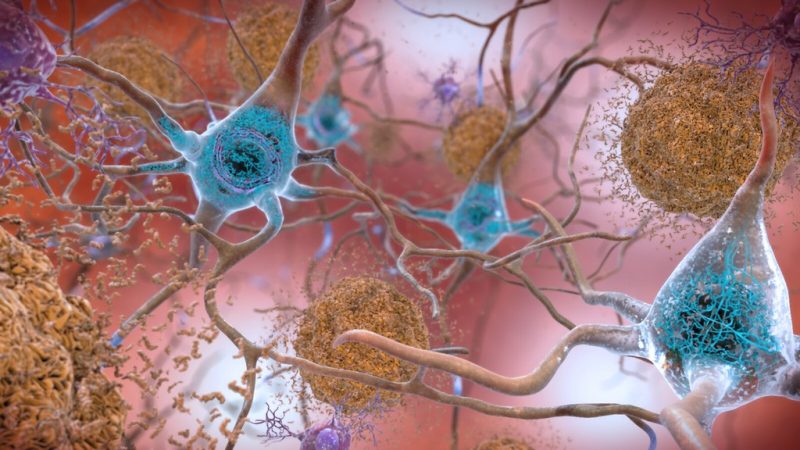
The key to understanding this terrible disease, and maybe even finding new treatments, lies in the science. It’s commonly known that memory loss and some form of dementia is common with aging, yet we don’t know why. A fairly recent discovery poses that something called an amyloid-beta oligomer (ABO), a type of protein plaque, is found in clumps inside an AD brain, and might contribute to damage associated with AD. Here’s a basic rundown of ABOs in relation to damage:
Normally function to promote healthy brain growth as proteins called AB40
Formed by enzymes called secretases
With age, mutations occur in genes that lead to creation of abnormal AB42 proteins
The ABO hypothesis is only one possible pathway that can accelerate damage. Another involves a brain protein, called Tau. In this pathway, Tau proteins are irregularly modified by enzymes, so they contain extra phosphate groups, and form tangles to complement plaques. Quite literally, AD brains are “dirty,” but human brains lack the means to properly clean them up! But how do enzymes go out of whack in the first place?
Before trying to answer that question, let’s look at a disease that’s seemingly has nothing to do with AD – type 2 diabetes (or T2D). Unlike Alzhiemer’s, T2D has some attributed causes, most linked to poor exercise habits and excessive sugar intake. Notable symptoms include:
Increased thirst and urination
Hunger
Weight loss
Fatigue
Trouble healing
For a full list of symptoms, risk factors, and tips for prevention, the Mayo Clinic page is available (here)
T2D has many implications, but in relation with dementia we must focus on how it impacts a specific hormone – insulin. Just like AD, an understanding starts with – you guessed it – science. When you eat a meal, your blood sugar goes up. In response, your pancreas will release insulin to signal all your body cells to take up this extra sugar, or glucose, from your bloodstream. But when there is consistently excessive sugar intake and a lack of physical activity (which normally stimulates the use of glucose), the body might become resistant to its own insulin, or it might produce less, for reasons we’ll explore later. This means the body is less able to store glucose and use it, producing the metabolic symptoms above.
In With Insulin – Bridging the Gap Between AD and T2D
Is insulin the missing link? We can try to bridge the gap between AD and T2D using what we know about insulin resistance. A skim of this review paper offers brilliant insight on exactly how insulin links a brain disorder with a metabolic disorder. To summarize its objective in three statements:
T2D has long been recognized as an underlying risk factor for developing T2D, and vice versa. Both conditions affect millions of people worldwide, and both social and financial implications are likely, as there is currently no successful means of treatment.
Understanding the key molecular mechanisms that link the two pathologies together are crucial to the development of potential treatments, but to this day are still under study.
Therefore, understanding existing research on mammalian models and identifying molecular-level mechanisms of pathogenesis in both diseases is crucial to both medicine and the scientific community.
Sounds complicated? Well it is, but we can start by learning how insulin functions in the brain. Insulin receptors, as mentioned above, are found nearly everywhere in the body, and the brain is no exception. Small amounts are even synthesized in the brain, in (surprise!) the areas important for forming and storing memories, such as the hippocampus. Aside from its metabolic use, insulin signalling serves to protect brain cells, maintain and balance neuron growth, and promote synaptic plasticity (a fancy word for how neurons change to allow for memory formation), via a variety of chemical cascades. An overview of the molecular insulin signalling pathway is visualized in the video below:
Or if you’d rather read:
Insulin binds to an insulin receptor.
A phosphate group is added to an amino acid called tyrosine, located on the receptor.
The receptor proceeds to add phosphate groups to tyrosine on Insulin Receptor Substrate (or IRS proteins – not the Revenue Service).
Adding a phosphate to tyrosine is like an “on switch,” and the IRS protein team goes on to act on multiple pathways that can trigger changes in gene expression and thus brain changes listed above.
IRS action can be “switched off” when a different amino acid on IRS – serine – gets a phosphate. This stops insulin signalling.
So T2D leads to insulin resistance, and less response to insulin means the hormone can’t do its work in the brain. T2D causes alzheimer’s, right? Though that might be part of the equation, this becomes a classic example of the chicken and the egg – since both diseases increase the likelihood of developing each other, which one comes first? Luckily, there are several proposed pathways that might aid in our understanding:
Inflammation: Remember those microglia mentioned before? AD is characterized by chronic, low levels of inflammation in the brain, likely due to microglial response to ABO plaques. Likewise, in T2D and obesity, accumulation of adipose (fat) tissue promotes inflammation. When there’s inflammation, immune cells release chemicals called cytokines (primarily a type called TNF-alpha). Not only do these promote more inflammation when they bind with cytokine receptors, but they can also shut off insulin signalling by activating the “serine off switch.” In summary, inflammation brought about by both AD and T2D leads to cytokine release, which can promote insulin resistance, which exacerbates both metabolic symptoms and problems in brain function.
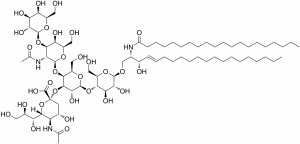
Gangliosides: This funny-sounding word is the name for a molecule (the big one shown here) normally found in cell membranes, notably in neurons. Gangliosides are located in regions of membrane called “microdomains” (quite literally, mini domains). A ganglioside called GM3 is elevated in diabetes, and has been found to disrupt the interaction between insulin receptors and IRS and promote the cytokine-induced resistance described above. Another ganglioside, GM1, decreases GM3 metabolism and can also build up in membranes. Interestingly, GM1 promotes the aggregation of ABOs seen in AD, so more of it leads to more plaque build up, which triggers more inflammation, and the vicious cycle continues! This seemingly simple molecule offers another link between T2D and AD. The only gaping hole is – we don’t currently know why gangliosides become elevated in the first place in T2D.
mTOR: mTOR is a protein normally responsible for cell growth control and regulation. mTOR is a complex topic, and it can be hard to discuss its function without entering the weeds of scientific papers. To oversimplify things a bit, if mTOR is incorrectly activated at any stage of development, developmental and memory problems can occur in the brain. It’s thought that too much mTOR activation leads to insulin resistance by, again, promoting the infamous activation of the “serine off switch” on IRS, by interacting with another protein called S61K. And alas, AD patients are often found to have higher amounts of mTOR! Then again, we don’t know why mTOR goes crazy in the first place. Nonetheless, another link, another connection.
After exploring the complex links that exist between these two terrible diseases, is it even possible to try and come up with new treatments, whether for diabetes or Alzhiemer’s? Science is still a long ways from finding an end-all-be-all solution to cognitive decline and insulin resistance, but some of the pathways above offer potential (and quite unexpected) means of therapy:
Insulin – Starting with the hormone itself. Not only is it used to treat T2D, but administering insulin has been found to boost cognitive effects in previous studies
Immunosuppresors – Though not ideal, immunosuppressors can reduce immune cell and potentially microglial activity, which could mean less cytokines and inflammation
Ganglioside targeting drugs – Less gangliosides means less plaque formation, less inflammation, and so on. Studies have found better cognition after using drugs that decrease levels of GM1
Methods of mTOR inhibition – Drugs that inhibit mTOR could decrease its effects, boosting cognitive performance.
One target that is worth taking note of is PtP1B, as it is thought to be involved in both AD and T2D. Protein tyrosine phosphatase 1B is an enzyme that is normally involved in regulating insulin signalling. It decreases insulin signaling by removing the phosphate “on switch” from tyrosine on both the insulin receptor itself and from our friend, the IRS protein. PtP1B also decreases signalling from a molecule called leptin, which is quite similar in function to insulin in its function within the brain, and also promotes the metabolism of harmful ABOs. To make things worse, PtP1B also inhibits brain derived neurotrophic factor (BDNF), a chemical important for making new neuronal connections and learning. It’s no wonder PtP1B is found at increased levels in Alzhiemer’s patients! This information has led scientists to look at ways to decrease PtP1B activity as modes of treatment.
Getting back to the nagging question, is Alzhiemer’s really another form of diabetes? To keep it short, we don’t really know. But advancements in the scientific and medical communities can be made by understanding how both diseases play into each other. It may be a while before we see treatments that can slow, or even halt, the progression of both types of diseases all together. But like all things in science, great discovery must start with even greater inquiry.
For more information about alzhiemer’s, you can check out this organization here
Schizophrenia is a mental disorder in which people interpret reality in an abnormal way. But who is to say experiences of another are abnormal? Patients with schizophrenia may show positive or negative symptoms. Many times patients do not notice if their symptoms are causing them to perform in abnormal ways. Is treatment worth it if it negatively impacts quality of life? Maybe society needs to do a better job at accepting people for who they are instead of automatically assuming a person needs treatment. It’s a big question without a clear answer. More research must be done to see what specific pathways can be targeted to reduce symptoms and improve quality of life. In this blog, we will look deeper into the symptoms of schizophrenia and some of the research done on the signaling pathways that may be involved in the occurrence of these symptoms.
What is considered abnormal?
Many different types of symptoms can be present in patients with schizophrenia. These include positive, negative, and cognitive symptoms.
Positive Symptoms: delusions, hallucinations, thought disorders, psychomotor problems
Negative Symptoms: Loss or reduction in the ability to initiate plans, speak, express emotion or find pleasure in life; many times mistaken for laziness or depression
Cognitive Symptoms: problems with attention and memory; most disabling for patients trying to lead a normal life.
All of these symptoms may be abnormal, however, it must also me remembered that it is all on a spectrum. Symptoms may be noticeable, but they may not be affecting the patient’s quality of life or are threatening to the people around them. If a patient is experiencing hallucinations, who is to say that hallucination is affecting them in a negative way? Maybe the hallucination is a support system that is necessary for the person’s everyday life.
What is going on in the schizophrenia brain?
Schizophrenia is a brain development disorder. Current treatments do not focus on the underlying mechanisms involved in schizophrenia. These mechanisms involve the Wnt signaling pathway.
Wnt pathway à Schizophrenic Symptoms: When a Wnt ligand does not bind to the receptor, the intracellular destruction complex continues to exist. This complex keeps Beta Catenin phosphorylated thus decreasing the concentration of Beta Catenin. This leads to no transcription within the nucleus.
Wnt pathway à No Schizophrenic Symptoms: When a Wnt ligand binds to the receptor, recruitment of proteins facilitate the dissociation of the destruction complex. This decreases phosphorylation of Beta Catenin, which increases stability in the cytoplasm and increases translocation of Beta Catenin into the nucleus for where Wnt producing genes are activated for further transcription.
To simplify these pathways, Beta Catenin must enter the nucleus to cause gene transcription. Without transcription of Wnt dependent target genes, symptoms of schizophrenia may occur.
Treatment?
With this research, we know the destruction complex plays a critical role as to whether or not Beta Catenin enters the nucleus to cause gene transcription. More research must be done to exactly pinpoint the area pharmaceuticals should target.
The bigger question to me, however, is when to know when treatment is necessary. Treatments today do not specifically target the Wnt pathway and often cause detrimental side effects that dampen a person’s quality of life. Before resorting to pharmaceuticals, I believe holistic approaches may be more beneficial to get a full understanding of what the patient with schizophrenia is going through. This may involve one-on-one therapy to get an idea of the emotional, psychological, social, and physical aspects that may come along with schizophrenia.
For more information on the research done on Schizophrenia and the Wnt Pathway follow this link:
Everyone remembers the celebrations, such as weddings and parties, where your friends and family gather to have the time of their lives. We remember the events that bring joy to our life. Unfortunately, we also tend to remember those ‘not so fun’ events that may cause stress and/or anxiety in our everyday lives. Many of us can remember where we were when we heard about the events on 9/11. However, you probably don’t know where you were on 9/10.
Many times we wish we could erase some of these past stressful events from our memory and instead remember more of the events that have escaped from our recollection. However, our brain’s wiring and decisions on what to remember has its benefits.
It is an evolutionary phenomenon for our brains to recollect past events. We learn from our mistakes. However, many times the emotional load of past events may cause stress and/or anxiety that affects our everyday lives. In some situations, our memories that carry along strong emotions with them can become pathological, such as in posttraumatic stress disorder (PTSD) or Generalized Anxiety Disorder (GAD).
How stressful memories can lead to disorders in the brain:
Pathways involving glucocorticoid hormones (aka steroid hormones) and altercations with gene transcription impact the formation of memories.
The function of memory consolidation is heightened by glucocorticoids. During a stressful event, these stress hormones are released. Pharmacological testing has been used to determine which specific receptor leads to an adaptive response to a stressor. This was achieved by inhibiting glucocorticoid receptors found in the dentate gyrus region of the hippocampus. It was found that these receptors did not produce the adaptive response of quickly immobilizing when inhibited. Thus, glucocorticoid receptors in this region of the brain are involved in response to stressful events.
Also found in the dentate gyrus region of the hippocampus was a high quantity amount of altered proteins known as the H3S10p-K14ac histone. This histone wraps up DNA and increases the expression of “immediate early genes” such as c-Fos and Egr-1.
c-Fos: involved in long term changes for adaptive behaviors
Egr-1: important for memory formation and learning
These proteins are directly involved with forming strong memories and consolidation processes as well. This underlying mechanism can thus cause an increase of “noisy” thoughts that are characterized with the intense memories of the stressors.
What does this all mean?
The dentate gyrus plays a pivotal role in the encoding of information and the H3S10p-K14 histone plays a central role in kick-starting gene transcription required for long-term changes in neuronal function. As of right now, treatments of PTSD involve medications commonly prescribed for anxiety. However, there is a difference between these disorders. More research on the stress response and the formation of strong memories could potentially advance the treatment methods for PTSD.
We only sometimes remember the good and the bad, but we almost always remember the ugly. How can we control the effects these ‘ugly’ memories have on us, yet still remember the ‘good’ memories? It’s a question where much more research is needed, but the research presented is a good start!
For more information on the research presented follow this link:
Many of us may know of someone who has suffered from either Type II Diabetes or Alzheimer’s. Maybe you even know of someone who suffered from both. Did you ever think that there could be a link between the two?
Type II Diabetes nearly doubles the risk of dementia. Conversely, Alzheimer patients have an increased risk of developing Type II Diabetes. These two diseases are also on the rise, likely due to the increase in unhealthy eating habits seen across the globe.
Making unhealthy choices today can lead to an unhealthy brain later in life. The evident connection between Type II Diabetes and Alzheimer’s shows us why it is important to adopt a healthy lifestyle. The remainder of this post will describe the evidence found between these diseases.
WHAT’S THIS ALL ABOUT? – INFO YOU NEED TO KNOW
Type II Diabetes: Many times due to unhealthy eating habits, our bodies over time can become to the insulin that is being produced in our bodies. Once this ability is lost, insulin is unable to respond to increased blood sugar levels. Because of this resistance, our bodies cannot make enough insulin to keep blood sugar normal/lower blood sugar levels. Therefore, the body can no longer send insulin to tell cells to store the sugar and a buildup of sugar is found in the bloodstream. Symptoms of Type II Diabetes may include:
increased thirst and urination
increased hunger
tiredness
blurred vision
neuropathy
weight loss
Alzheimer’s: The most prevalent form of dementia, Alzheimer’s causes memory loss due to cerebral atrophy and a buildup of neurofibrillary fibers and amyloid beta oligomer (ABO) plaques. These physical detriments can be caused by a number of factors, many of which can also be related to Type II Diabetes, such as:
Neuro-inflammation
Abnormal ganglioside metabolism
Deregulated mTOR signaling
***the science for these factors will be described below
WHAT’S THE CONNECTION? – THE SCIENCE BEHIND IT
Insulin resistance, as seen in Type II Diabetes is a result of chronic inflammation in peripheral tissues due to an increased amount of fat tissue. Brains with Alzheimer’s also have increased levels of inflammation compared to a healthy brain. Sustained inflammation causes the recruitment of macrophages and local secretion of proinflammatory cytokines. Secretion of these cytokines induce insulin resistance. Once these cytokines are released in the brain through neuro-inflammation, ABOs can bind to them causing the plaque formation.
Insulin receptors are involved in many major pathways in the brain. Microdomains allow for cells to perform different signaling tasks based on their location. Gangliosides are commonly associated with these microdomains and facilitate reactions such as the transformation of a single ABO molecule to a plaque formation. With too many ganglioside reactions occurring, they will begin to displace insulin receptors in the brain, thus contributing to insulin resistance.
mTOR, a serine/threonine kinase, is critical for the development of the cerebral cortex. Increased activation of the mTOR pathway can lead to neurodegeneration and insulin resistance. This may be due to the buildup and hyper-phosphorylation of the tau protein, which binds and stabilizes the microtubules found in the neuron. An increased amount of tau protein is found in both Type II Diabetics and Alzheimer patients. Tau makes up the neurofibrillary tangles once it detaches from the microtubules and finds another tau molecule to bind to. This buildup forms tangles inside the neuron and the neuron loses support, shape, and integrity. Therefore, an action potential is unable to be successfully carried out.
SO… TAKE CARE OF YOUR BODY!
Our choices we make today regarding how we treat our bodies will affect us somehow in the long run. Will that be a positive or negative effect? You get to choose! Let the correlation between Type II Diabetes and Alzheimer’s that has been described above influence you choice. A healthy brain for life starts today!
Follow these helpful links to learn more about the importance of maintaining a healthy brain:
Schizophrenia is easily one of the most recognizable psychiatric disorders. However, the disease is more complicated than people believe. First, there are two categories of symptoms: positive and negative symptoms. Positive symptoms are the more famous of the categories. These include symptoms like hallucinations and delusions. Negative symptoms include withdrawal and a sort of “flatness” or “coldness” in expressing emotion.
The exact pathology of schizophrenia is unknown, though there are several theories. Infections during pregnancy likely play a role, making schizophrenia a developmental brain disorder rather than a traditional psychiatric disorder. There is also some genetic factors, mainly involving extra or missing copies of various genes.
One possible mechanism for schizophrenia involves the Wnt pathway. Wnt is a signaling molecule that connects the LRP5/6 protein to the frizzled protein. This activates the disheveled or Dvl protein. Meanwhile, the protein beta catenin is normally bound up in a protein complex. When Dvl is activated, it frees beta catenin from this complex. Beta catenin can then enter the nucleus and bind to DNA. Here, it ensures that the transcription factors (factors that aid in the creation of RNA and eventually proteins) TCF/LEF bind to DNA and make proteins. All of this can be seen in the picture below. [1]
Schizophrenia involves an increase in dopamine. Dopamine binds to the D2 receptor, which in turn activates the enzyme Akt. This enzyme stops the inhibition of GSK3 beta, one of the proteins in the complex that holds beta catenin at bay. Since GSK3 is more active, beta catenin is less active, making it unable to reach the nucleus.
A lot of this information has been found without directly experimenting with schizophrenia. It is not really possible to give an animal schizophrenia. Most of this information comes from studying the exact effects that anti-psychotics have on the brain and studying animals that have a modified Wnt pathway.
Most people have likely heard of schizophrenia. It’s the disorder with the hallucinations right. But, few people have actually experienced it. Schizophrenia affects around 1 percent of the world population and about 1.2 percent of the United States population, that’s about 3.2 million people.[i] Since it’s not as common as general anxiety disorder or major depressive disorder, schizophrenia doesn’t get studied as much and there are fewer drugs on the market for it. Those that are on the market often have harsh side-effects. Today’s current antipsychotics are on the right tract in terms of targeting the Wnt pathway. Lithium also targets the Wnt pathway, but isn’t typically prescribed for schizophrenia, or even bipolar disorder. From this, it would seem that there’s a need for different drugs used to treat schizophrenia, but there’s a belief about the lack of demand. However, just because a disorder is rare doesn’t mean it isn’t worth studying. Three point two million people is still a lot of people and for many this disorder is very real.
In the conclusion of the An Emerging Role for Wnt and GSK3 Signaling Pathways in Schizophrenia, KK Singh discusses how schizophrenia is complicated and hard to replicate in the laboratory, especially in animal models. This phenomenon does give science some hope. We may not be able to give animals schizophrenia, but we can play around with this pathway to induce schizophrenia-like symptoms, allowing us to better study it. However, this should not deter us from studying it. If anything, it should challenge and inspire us.
Post-traumatic stress disorder (PTSD) is a complicated psychological disorder. While typically associated with army veterans, the disorder is actually common among people who have experienced other horrors, like heinous crimes or natural disasters. What follows is a traumatic reliving of the event. People with PTSD may experience flashbacks, nightmares, unwanted thoughts or memories, and a sense of general anxiety. Symptoms can appear immediately after or may take years to appear. To make things worse, people do not always seek help after the traumatic event, allowing symptoms to worsen.
According to Johannes M.H. Reul, PTSD is really a negative side effect of human’s amazing ability to create strong associations. People associate what would be a neutral stimulus so strongly with a traumatic memory that it impairs daily functioning. However, there is hope to this. PTSD is associated with memory and memory has a biological pathway.
When we experience a stressful event, our bodies release corticosterone. Corticosterone then binds to glucocorticoid receptors (GR). GR then activates extracellular receptor kinase (ERK). Activated ERK can do one of two things: activate mitogen stress kinase 1 (MSK1) or activate Elk-1 by removing a phosphate. Eventually, it will do both.
You might remember from your biology class that our DNA is very long, so long that if all the DNA in your all of your cells was stretched out it would wrap around the solar system, twice![i] To keep our cells to a reasonable size, DNA is wrapped around molecules called histones and condensed into structures called chromatin. MSK1 and Elk-1 unroll DNA (though not all of it at once). This allows for transcription, which makes proteins c-Fos and Egr-1. These proteins work closely with a variety of other mechanism like the NDMA receptor in order to create associations.
While c-Fos and Erg-1 work with NMDA receptors, the NDMA receptor is also part of the memory association process. Glutamate binds to NMDA receptors. This adds a phosphate to MEK, which in turn passes it on to ERK.
Fig. 1. Above is a diagram from the article that outlines the mechanism of memory association.
All of this takes place in specialized neurons within the hippocampus. These neurons are called granule neurons. Unlike neurons in other regions of the brain, these can die off and divide. This is great news for making new memories and associations.
All of this science was discovered very recently, within the last 30 years. Scientists first began to study this mechanism in the 1980s, but it was not until the early 2000s did they finally identify a mechanism. Most of the research was done using mouse models. However, you cannot really give a mouse PTSD. Though, we can identify and induce anxiety in mice. Since anxiety is a symptom of PTSD, we can use anxiety in mice to study PTSD and related disorders.
There are several ways to induce anxiety or stress in mice. One common way is the swim test. A mouse is placed in a pool that has no exit. The mouse frantically searchers for an anxiety, but eventually realizes that there isn’t one. The mouse then goes limp and helpless before being scooped up by a researcher. Mice who undergo this test multiple times eventually spend less time swimming. This retesting is highly dependent on stress hormones. Mice who were given blockers to GR receptors spent more time swimming in the retest[i].
Implications
The article is very technical in its nature and in the descriptions, likely because Johannes M.H. M. Reul were only discovering the pathway, not a connection or implication like other articles discussed on this blog. The authors mention that it took them nearly three decades to find this pathway. This is fairly new science, so it is difficult to pinpoint the exact implications of this study.
Since we know the pathway, it seems plausible to create a drug that acts on an element of this pathway, therefore eliminating or preventing PTSD. However, that is likely not possible. All of this transcription process happens very quickly, less than 15 minutes after the event. People who suffer from PTSD often are not aware of or get treatment for their symptoms until months or years after the event.
Additionally, there is also an ethical side to this. While stress can be bad, it is essential for learning. I’m sure we can all think of a time where we learned something through stress. There is even a common phrase for it in the English language: “learning something the hard way.” Creating a drug that acts on this pathway could have unintended consequences and limit a person’s normal ability to learn. It would be better to have a patient relearn and un-associate everyday things with the traumatic memory.
PTSD is unique among psychological disorders in that it has a direct cause. Disorders like depression and generalized anxiety disorder can affect anyone and be triggered by a number of different things. PTSD is always triggered by some traumatic event. This makes it difficult to study. We cannot expose people to a traumatic event and study them afterwards. This is bad for two reasons: first, we cannot expose anyone to a psychologically harmful event for ethical reasons and second, not everyone who experiences a traumatic event shows signs of PTSD. Exactly why some victims of traumatic events get PTSD and some do not is currently unknown. Women in general are more likely to get PTSD, but this maybe due to the fact that women are more likely to be victims of crimes like rape and assault. We know that there is some genetic basis for anxiety (a common symptom of PTSD and the one symptom that researchers used in testing), so there may very well be some genetic factor with PTSD. However, there is not much that can be done to prevent, except stopping the traumatic events that cause PTSD like rape, war, and assault.
Overall, PTSD is a unique psychological disorder. The disorder is really a side-effect of human’s amazing ability to make associations. However, these associations become so strong that it affects our everyday functioning. It is difficult to study treatments of it because we cannot ethically give a human PTSD. We can induce anxiety in animals, but this is not entirely the same as PTSD, but a mere symptom of it. However, we ought not to shy away from studying disorders like PTSD simply because they are complicated. If anything, their complications show us something about the human condition. We are so good at making associations and learning that sometimes it harms us. But, there is no reason that this amazing ability cannot be used fo
[i] Johanes M. H. M. Reul. Making memories of stressful events: a journey along epigenetic, gene transcription, and signaling pathways. Frontiers in Psychiatry. Vol. 5. Jan. 2014.
Schizophrenia is a neurodegenerative disease which has often been portrayed through various forms of media. However, this depiction is often a misrepresentation of the disease. Movies and tv shows often portray the disease as making an individual very aggressive, delusional, allows them to hear voices, and all around crazy. Although some of these are symptoms of the disorder, this stigma does not nearly encompass the whole disease. Schizophrenia is very complex and still not very well understood by the scientific community. Symptoms span a wide range and often differ dramatically between individuals leading to various treatment options. Current research has shown how each of these treatment options is closely related to the Wnt pathway and Wnt signaling. By better understanding how each of these treatment options affects the Wnt pathway and subsequently schizophrenia, scientists are obtaining a more complete understanding of the disease and breaking down the stigma created by the media.
As previously stated, the symptoms of schizophrenia vary dramatically. According to the Mayo Clinic website symptoms of schizophrenia involve delusions, hallucinations, disorganized thinking and speech, disorganized or abnormal motor behavior or negative symptoms. Negative symptoms are those that reduce the ability to function normally. Examples are lack of personal care and disinterest in everyday activities. These negative symptoms often lead to a misdiagnosis of the disease, as many of these symptoms resemble other neurodegenerative diseases such as depression. Of great importance is the time at which symptoms of schizophrenia begin to manifest as this usually affects how the disease is expressed. For example, symptoms in teenagers are a withdrawal from friends and family, drop in school performance, trouble sleeping, and lack of motivation. These symptoms, which can often be diagnosed as depression, are a far cry from the media’s depiction of the disease. Only by accurately displaying and discussing the disorder can the stigma surrounding the disease finally be torn down. Scientists are also attempting to break this stigma by learning more about this complex disorder. By examining how current treatments affect the disease with respect the Wnt pathway scientists are discovering vital information thus breaking the stigma.
One of the main methods for treating schizophrenia is through the use of psychiatric pharmaceuticals. Many of these small molecule drugs often directly or indirectly target Wnt signaling. One such molecule is dopamine (DA). DA signaling has been shown to inhibit Akt which inhibits GSK3. If GSK3 is not phosphorylated, then b-catenin cannot enter the nucleus and allow for proper gene transcription. Not having proper gene transcription can lead to the degeneration of neurons thus leading to an increase in neurodegenerative disease such as schizophrenia. However, DA pharmaceuticals are not the only drugs used to repress schizophrenia. Lithium has also been used as a viable treatment option. Lithium directly inhibits GSK3 activity by competing with magnesium as well as indirectly inhibiting it by increasing the inhibitory phosphorylation of GSK3. This leads to an accumulation of b-catenin, which leads to proper gene transcription thus allowing for proper cell growth.
Scientist are not only working on treatments for the disease but also working on identifying potential genes which could lead to the disease. Current research has shown that genes such as DISC 1. DISC 1was first identified in a multi-generation Scottish family that suffered from schizophrenia, bipolar disorder and major depression. Since its discovery DISK 1 has been found to regulate the stability of b-catenin through GSK3, resulting in better gene transcription. Further studies are currently being done to identify other genes which can could lead to the manifestation of this disease.
The stigma surrounding schizophrenia resembles a crazed individual who hallucinates and is plagued by voices in his or her head. However, this is not an accurate representation of the disease. Schizophrenia is very complicated its symptoms manifest itself in a variety of ways. Currently scientists are learning more about the disease in an attempt to break the stigma and help enlighten the public. Only once this misconception is broken can individuals struggling with the disease come forward without fear of humiliation or ridicule.
If any of you were akin to me in your middle childhood, you were probably instructed to NOT do something regularly. The probability that I would listen to such demands was low, sadly very low. However, after feeling the punishment of not listening, either from a natural event or a disgruntled parent, I learned quickly to not engage in such an event again. The formation of memories allows us to grow and learn form painful experiences. What happens however, when such strong memories form from mundane events? This is were anxiety disorders such as PTSD can manifest. There are several neurological factors which are thought to cause these overactive memories and thus lead to a variety of anxiety disorders.
Glucocorticoids
One important factor that can contribute to the overactivation of strong memories are glucocorticoids. These hormones, which are often associated with fear and stress, have been to form a complex for with other enzymes in the brain thus allowing gene transcription leading to the formation of memory. Tests with various animal models show that animals treated with glucocorticoid agonists struggle much longer under various conditions instead of learning quickly from previous events. This leads to the conclusion that these glucocorticoids could be overactive in a variety of anxiety disorders thus producing strong memories from very mundane situations. The diagram below does a nice job of demonstrating how these glucocorticoids help in gene transcription.
The Role of the ERK/MAPK Pathway
It would be foolish to only discuss the role of glucocorticoids when the figure above also shows how the Erk/MAPK pathway involved in the formation of memory as well. In fact, both of these pathways must happen in tandem for the proper transcription of genes and thus memory formation. Since the Erk/MAPK pathway has already linked to learned behavior it makes sense that it may also play a role in memory. A series of studies found that a NMDA receptor agonist strongly inhibited the learning process during forced swim tests of rodents. In other words, the inhibition of the Erk/MAPK pathway prevents the formation of the glucocorticoid receptor/ERK complex, which in turn cannot phosphorylate MSK-1and Elk-1. It stands that if these two kinases cannot form then there can be no gene transcription which leads to a lack of memory consolidation. However, if the ERK/MAPK pathway is overactive you can have the over activation and phosphorylation of MSK-1 and Elk-1 which leads to the transcription of genes for mundane events.
Conclusion
The formation of memories is vital to not only our learning but also our survival. Memories can be formed through several pathways however, the formation of strong and or painful memories often occurs through the ERK/MAPK pathway along with glucocorticoids. It is thought that the overactivation of this process can lead to a variety of anxiety disorders, including PTSD. There are other aspects to be considered, such as the role of the amygdala and hypothalamus, both of which have been shown to play a role in anxiety. It is imperative that each these factors be more thoroughly examined in order to one day find a cure for those suffering with anxiety disorders.

















{kind=link}