*About (See that’s the concussion doing it’s thing)
For this blog, I will again include potential symptoms as well as neuroscientific aspects behind concussions. However, I first want to focus on some other information provided to me by a friend currently dealing with a concussion. Hopefully this will prove to be equally, if not more, beneficial to you. Wishing her a steady recovery, here are 10 things my friend wishes people knew about concussions:
- Every concussion is different. One experience (maybe your own or one that you’ve heard about) is not necessarily generalizable to others’ experiences. It’s really hard to understand what it’s like until you’ve had one.
- It may be a moot point, but you can’t see concussions. Therefore, even if someone seems fine, it doesn’t necessarily mean that they are.
- Concussions make everything harder, especially because they never really “turn off” and your head constantly either hurts, has pressure, or feels foggy. While it varies from person to person, concussions can make reading, seeing, writing, listening, thinking, sleeping and, therefore, just existing hard. It makes you feel helpless.
- Have compassion, be patient, give endless amounts of love. Having a concussion can make people feel isolated and alone because they have to spend a lot of time in quiet environments, which can often mean by themselves. For people in your life who struggle with mental health, all of that forced alone time can especially take a toll.
- Be there for your loved ones with concussions, but try to avoid frequently asking “How’s your head?” or “How are you feeling?”. Of course, it’s important to show that you care and to let them know that they can talk to you about their struggles any time. But on the other hand, they are constantly dealing with their concussion and probably would appreciate a different topic of conversation once in a while!
- Instead of making people feel guilty, be conscious of people’s concussions because they have no control over the symptoms. Trust that they are fighting and handling life as best they can, even though you may not see it. They are probably already pushing their brain to do more than it should. It’s not their fault that they are not able/ supposed to do certain things (like use technology, watch movies, or be in a loud environment).
- Concussions are not about “just working hard” and “pushing through”. Pushing through is painful, not productive and not helpful in the recovery process.
- Symptoms can rapidly and unexpectedly change. Someone may be feeling alright one minute, but not so much the next. This can be applied to the recovery process as well because it is often not linear.
- Never make the person with the concussion feel like they need to “prove” their injury to you. Believe them. Especially when it has already been diagnosed.
- Support them. Love them. Hugs galore (if they like hugs).
After providing this advice based on personal experience, the information below covers some of the medical and scientific aspects of concussions.
Types, Causes & Symptoms
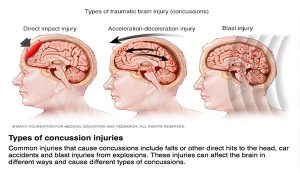
Causes of concussions are usually significant blows to the head or upper body, sudden acceleration or deceleration of the head, or blast injuries. These also mark the different types of concussions the brain can experience, depending on the nature of the event. Getting any one type of concussion can occur in a wide variety of circumstances.
Risks
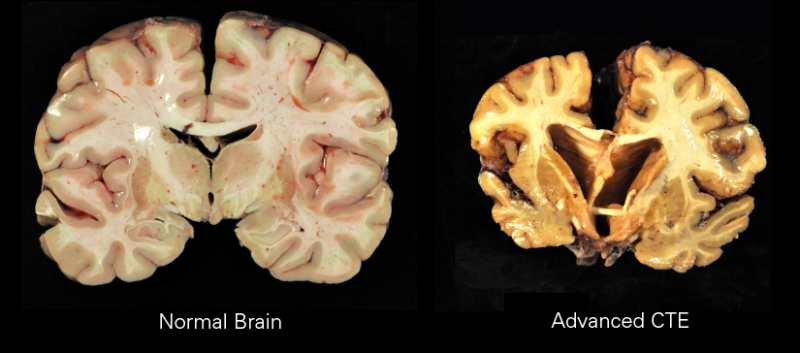
One of the circumstances in which concussions are most well known to occur is football. Lots of research has been conducted for this sport specifically (especially surrounding CTE), but contact sports in general (such as hockey, rugby, soccer, boxing, etc.) pose increased risks for getting a concussion. Furthermore, they are commonly diagnosed in the military as well from events as simple as falling to something as serious as bomb blasts.
Of course the general population can suffer from concussions due to falling as well, but also due to many other incidents like motor vehicle collisions, pedestrian or bicycle accidents, or physical abuse. Having had a concussion before also makes it easier to sustain a second concussion, while possibly making the symptoms more severe as well.
Symptoms
The symptoms and potential consequences of concussions are numerous and may include seizures, loss of consciousness, memory loss, nausea/ vomiting, headaches, mood changes (irritability, anxiety, depression), sensitive vision and hearing, difficulties with physical coordination, memory and concentration issues, lethargic or easily fatigued, trouble sleeping and waking up.
Science of Concussions
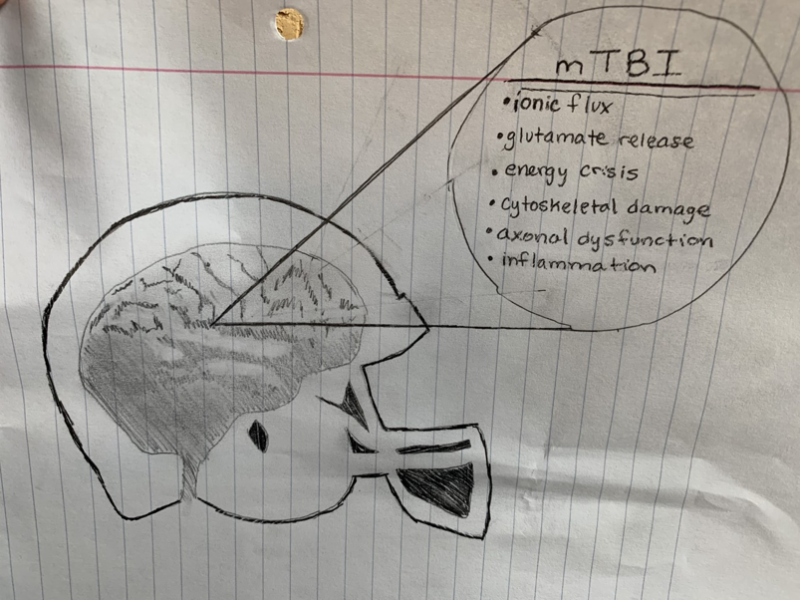
There are many different findings within concussion research as to what the biological/ neural expression of a concussion could look like. One such finding is that mechanoporation (small pores or defects in the membrane) can lead to potassium efflux out of and sodium & calcium influx into the neuron, as well as hyperacute indiscriminate glutamate release. This increased firing of neural cells can then lead to a “depression-like” state, where the firing is less likely, which could be the reason for some of the postconcussive impairments.
After this increased firing, ionic pumps are actively trying to restore ionic homeostasis of the cell. However, these pumps require energy in the form of ATP (adenosine triphosphate), which means that cellular storage is often strained or even depleted and hyperglycolysis occurs (increased glucose utilization two standard deviations above normal) in order to restore ATP levels.
Other pathologies can include cytoskeletal damage, which means that the structural integrity of neurons is lost and in severe cases can lead to axonal disconnection, leading to difficulties in axonal transport. Neurotransmission is also altered due to changes in the composition and function of glutamatergic NMDA receptor subunits. Under some circumstances inflammation and cell death can occur as well. For more information on the science click here.



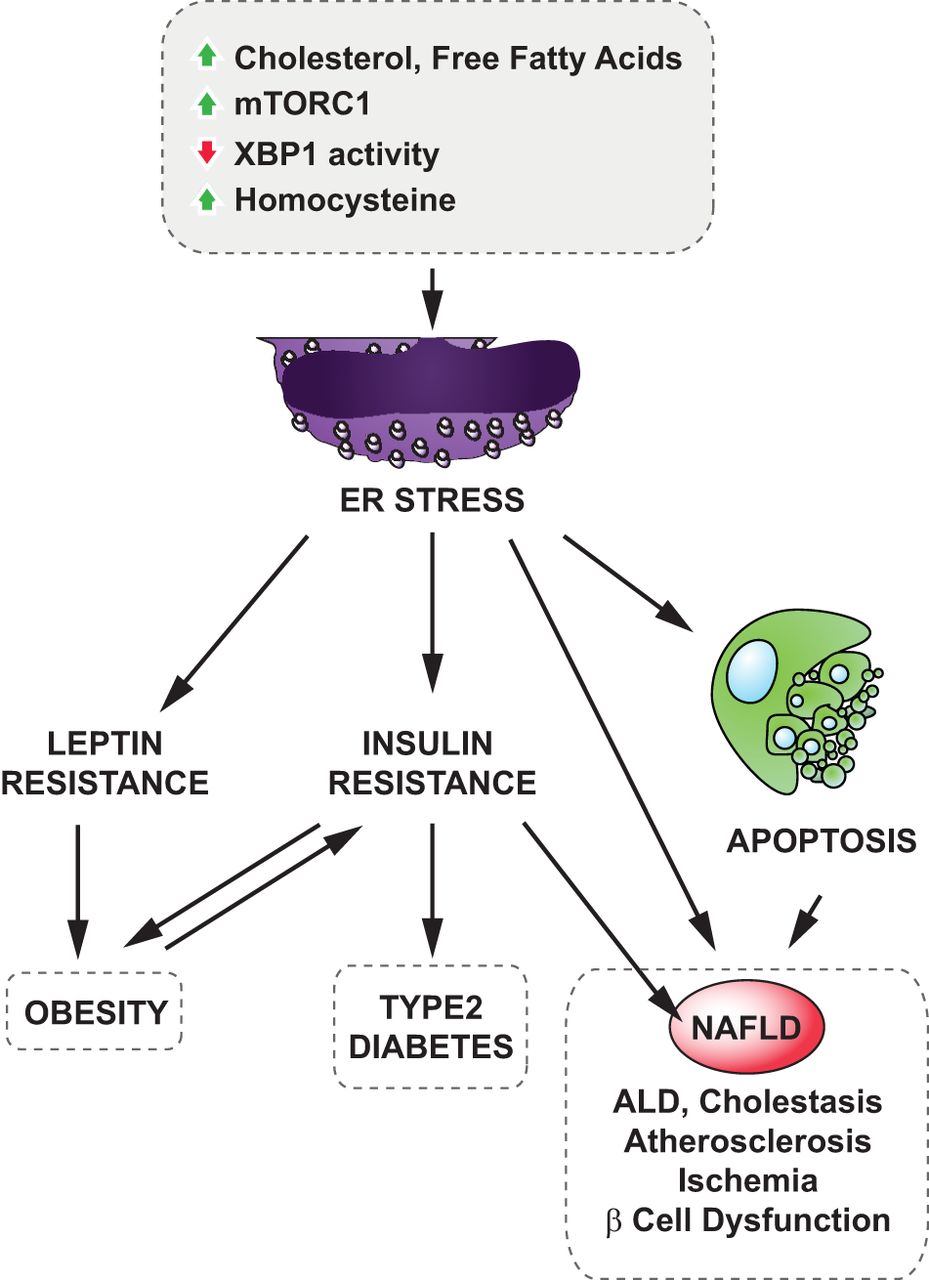
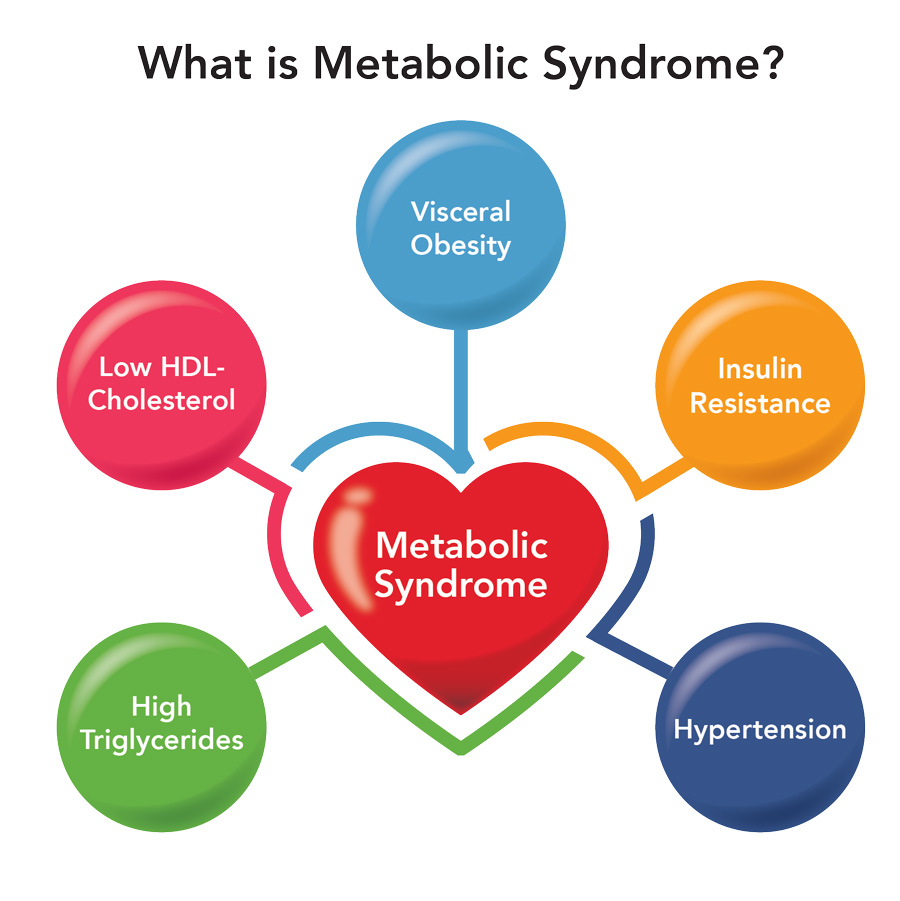 symptoms that lead to an increase in the risk of developing Type 2 Diabetes, Cardiovascular Disease, and stroke. The figure is a good graphic of what components are involved with metabolic syndrome. Having even one component of metabolic syndrome can increase your risk of development of a serious condition. About 1/3 of adults in the United States have metabolic syndrome. One of these components is critical in the hypothalamic inflammation that is seen in obesity, insulin signaling. https://www.mayoclinic.org/diseases-conditions/metabolic-syndrome/symptoms-causes/syc-20351916
symptoms that lead to an increase in the risk of developing Type 2 Diabetes, Cardiovascular Disease, and stroke. The figure is a good graphic of what components are involved with metabolic syndrome. Having even one component of metabolic syndrome can increase your risk of development of a serious condition. About 1/3 of adults in the United States have metabolic syndrome. One of these components is critical in the hypothalamic inflammation that is seen in obesity, insulin signaling. https://www.mayoclinic.org/diseases-conditions/metabolic-syndrome/symptoms-causes/syc-20351916


 lazy and eating food that is bad for them. While factors such as eating habits, exercise, and screen time all contribute to a person’s weight, so do medications, chronic illnesses, socioeconomic status, and access to healthy foods. Genetic predisposition has also recently been shown to play a major role in a person’s weight. What many people don’t know is that chemical changes in the brain are partially, if not largely, responsible for obesity and can be induced by outside factors.
lazy and eating food that is bad for them. While factors such as eating habits, exercise, and screen time all contribute to a person’s weight, so do medications, chronic illnesses, socioeconomic status, and access to healthy foods. Genetic predisposition has also recently been shown to play a major role in a person’s weight. What many people don’t know is that chemical changes in the brain are partially, if not largely, responsible for obesity and can be induced by outside factors.