It’s crazy to believe that I only have one semester left of my undergraduate career. Although it has been a few years since my first day at Concordia, I still remember it like the back of my hand. I remember the overload of information that I received during Orientation week: where campus resources were located, how to access campus mail, etc., but one thing I remember vividly was the constant mention of a four letter word: BREW.
I remember President Craft mentioning this word throughout his speech when he addressed the entire freshman class before we set out to volunteer in the Fargo/Moorhead community for Hand’s for Change. He stated something along the lines of, “At Concordia College, you will learn the meaning of Becoming Responsibly Engaged in the World, or BREW.” As a beanie-wearing freshman, I was eager to learn the meaning behind this daunting acronym, but to my surprise, I did not fully understand what it truly meant to BREW until I took Neurochemistry my senior year.
Specifically, Neurochemistry taught me how to BREW by teaching me what a liberal arts education is all about by helping me understand the five goals for liberal learning:
- Instill a love for learning
- Develop foundational skills and transferable intellectual capacities
- Develop an understanding of disciplinary, interdisciplinary and intercultural perspectives and their connections
- Cultivate an examined cultural, ethical, physical and spiritual self-understanding
- Encourage responsible participation in the world
I learned the beauty and purpose of each of these goals throughout this course, and I can’t wait to share them with you.
Neurochemistry was unlike any other class that I have taken at Concordia. I believe that what made this class so unique was it’s layout. The beginning of the year gave all of us the opportunity to develop a foundation in the basics of cell-signaling and the pathways that we would soon see at work as we dove into reading our weekly articles. Once it was time to start reading the articles, I quickly fell in love with how they were approached.
 We were given a week with each article: three entire class days structured something like this:
We were given a week with each article: three entire class days structured something like this:
(1) Monday: Come to class with the article read. When you read the article, try to gain an understanding of the main points, and come to class with questions about some aspects of the paper that you didn’t quite understand. The questions that you have will be the class’ assignment for Wednesday.
(2) Wednesday: Share your findings with the class: add your piece to help everyone understand the entire puzzle.
(3) Friday: Discussion leaders for that week will come prepared to talk about the topic more in depth. They will prompt you with questions regarding the disease/disorder in real life situations, and you will get the opportunity to hear the viewpoints of your classmates.
Fridays were the best days.
This was the only science class that I have taken at Concordia where learning wasn’t about memorizing facts and regurgitating them on a test. This class was about learning the science, and why it mattered.

Friday discussions gave everyone in the class a platform to discuss what was on their minds: their thoughts on the topic, how it made them feel, if they had a personal connection to it, and why they believed it was important to learn about. In no other science class are you given the opportunity to learn from your classmates in this way. This open communication not only strengthened my understanding of the topics that we covered, but it also made me dig deeper and think about topics in a new light.
These discussions allowed me to understand the first two goals of liberal learning:
- Instill a love for learning
- I fell in love with looking past the science printed on the page. I loved searching for the bigger meaning, the “why it mattered” to help contribute to discussions. As I begin medical school in the fall, I know that I will dig deeper and promote this type of communication with my new classmates, as I believe that it helped our class become more of a community where opinions were valued and ideas were encouraged to be shared. I know that this type of discussion will not stop after medical school, but will continue when I am a physician someday. I know that I will strive to have these deep conversations with my patients to help us build better relationships so that they can get the best possible care.
- Develop foundational skills and transferable intellectual capacities
- I believe that one of the most transferable skills that I will take from the discussions that we had in this class is the fact that personal opinions can be changed. It is so important to listen to others, and to remind yourself that you are not always right. I learned this time and time again throughout discussions when I would come with an opinion on a topic, only for it to be shattered and rebuilt by learning and listening from someone else’s perspective. Listening is such a powerful thing, and these discussions taught me how to actively listen to the opinions of those around me to gain a better understanding of my own beliefs.
In addition to learning in the classroom each week, this class also gave us the opportunity to make a difference in the community through a Community Action Project (CAP). The CAP not only allowed us to learn about issues in the community that we could help alleviate, but it also gave us the opportunity to discover the beauty of other disciplines outside of the sciences as we merged with social work students to complete the task.
This merging of disciplines gave me an insight into learning goal number 3:
- Develop an understanding of disciplinary, interdisciplinary and intercultural perspectives and their connections
I quickly learned as we merged with the social work students, that each of our classes had strengths and weaknesses to bring to the project. This interdisciplinary union helped me gain an understanding of when to be a leader and when to be a follower. We quickly learned that when the social work students had a strength, they would lead and we would follow, and vice versa. Not only is this strategy great for group projects, but it is very applicable to the real world. It’s often said that “teamwork makes the dreamwork,” and this couldn’t be more true. It is important to learn that everyone brings something unique to the table, and that no one has strengths in every area. We therefore learned that tackling a problem in the community was all about joining forces with those with differing strengths, so that the best outcome could be reached.
I gained an understanding of the last two liberal learning outcomes when we actually carried out our CAP.
- Cultivate an examined cultural, ethical, physical and spiritual self-understanding
The purpose of our CAP was to use musical interventions to enhance the quality of life for individuals with Alzheimer’s Disease, and we saw the music that we shared do just that. We partnered with Memory Café of the Red River Valley, and distributed the individualized plan of care that we developed as well as handmade CDs. As soon as one of the CDs began to play at a Memory Café event, an individual with advanced Alzheimer’s Disease immediately perked up and became more engaged in the craft that he was working on. Is there anything more fulfilling than knowing that something you were a part of helped someone? Even though this change may not seem like a huge difference to those of us without Alzheimer’s Disease, the music that that individual heard helped make his day better. I believe that this experience, and any other experience where you can help someone, is the best form of spiritual self-understanding. Isn’t that what life is all about? Leaving the world better than you found it? What could possibly be more fulfilling than that?
- Encourage responsible participation in the world

To put our CAP into perspective: we were able to positively impact the Fargo/Moorhead community. A bunch of college students enrolled in a capstone class changed the lives of individuals in our community because this class gave us the opportunity to. I don’t know about you, but knowing that something as unsuspecting as a school project could influence the community makes me wonder how else I could Become Responsibly Engaged in the World.
So what else do I have to say about this course? It changed the way that I viewed science. It made me want to become engaged in our world. It made me want to build better, stronger relationships with those around me. It pushed me to ask questions like “why” and “so what”. It made me a better person. I couldn’t recommend it enough. It was the perfect capstone experience.

 This love of learning was such an important part of this course. If I’m being honest, these four years of undergrad have been tough. As a chemistry and biology double major, I have spent endless hours going over material, reading, studying, doing homework… it has been a lot of work. And extremely stressful, as we constantly have our minds focused on what is ahead and how our grades will affect our future. I was starting to ask myself why in the world I ever wanted to be a science major. And then neurochemistry reminded me why. The excitement of finally discovering how a pathway works or how different molecules interact with each other reminded me that learning is not just about getting good grades. I found myself drawing connections from the papers we read to concepts I had learned during my years at Concordia. When you can finally apply what you have learned in the many biology and chemistry courses to “real life” topics such as neurological diseases, you begin to feel the value of your knowledge. Before neurochemistry, I felt as though I knew a bunch of random information about receptors and enzymes, but after this course I now realize how important that knowledge is. For this reason, I believe neurochemistry is the epitome of what a capstone course should be: it, for lack of a better term, caps off your college experience. It connects everything I have learned and showed me how my knowledge will be used in the field I wish to spend my life in. Neurochemistry was exactly the class I needed to round out my education and make me feel comfortable moving into the next stage of my life.
This love of learning was such an important part of this course. If I’m being honest, these four years of undergrad have been tough. As a chemistry and biology double major, I have spent endless hours going over material, reading, studying, doing homework… it has been a lot of work. And extremely stressful, as we constantly have our minds focused on what is ahead and how our grades will affect our future. I was starting to ask myself why in the world I ever wanted to be a science major. And then neurochemistry reminded me why. The excitement of finally discovering how a pathway works or how different molecules interact with each other reminded me that learning is not just about getting good grades. I found myself drawing connections from the papers we read to concepts I had learned during my years at Concordia. When you can finally apply what you have learned in the many biology and chemistry courses to “real life” topics such as neurological diseases, you begin to feel the value of your knowledge. Before neurochemistry, I felt as though I knew a bunch of random information about receptors and enzymes, but after this course I now realize how important that knowledge is. For this reason, I believe neurochemistry is the epitome of what a capstone course should be: it, for lack of a better term, caps off your college experience. It connects everything I have learned and showed me how my knowledge will be used in the field I wish to spend my life in. Neurochemistry was exactly the class I needed to round out my education and make me feel comfortable moving into the next stage of my life.




 During this course, we were able to rank topics according to our interests to form groups for a project that, throughout the semester, were going to work and engage the community in. I found the whole project inspiring, especially as it took the knowledge we learned in class and gave it a purpose outside of the course. Along with this, I found myself staying interested throughout this course as each week we tackled a new topic not for the goal of just learning it but engaging this knowledge to discuss the implications of what we had learned to medicine, the well-being of our community, and science.
During this course, we were able to rank topics according to our interests to form groups for a project that, throughout the semester, were going to work and engage the community in. I found the whole project inspiring, especially as it took the knowledge we learned in class and gave it a purpose outside of the course. Along with this, I found myself staying interested throughout this course as each week we tackled a new topic not for the goal of just learning it but engaging this knowledge to discuss the implications of what we had learned to medicine, the well-being of our community, and science. Working together with students studying Social Work during our Community Action Project helped us to build an interdisciplinary project. This was worthwhile, especially with my teams project focusing on mental health, as we had to focus on the science of mental health, but also the resources and supports important at our campus and in the community. During weekly discussions, we were also encouraged to answer questions posed by discussion leaders that often involved thinking about a variety of implications and perspectives.
Working together with students studying Social Work during our Community Action Project helped us to build an interdisciplinary project. This was worthwhile, especially with my teams project focusing on mental health, as we had to focus on the science of mental health, but also the resources and supports important at our campus and in the community. During weekly discussions, we were also encouraged to answer questions posed by discussion leaders that often involved thinking about a variety of implications and perspectives.
 As a capstone to my Neuroscience major at Concordia College, Neurochemistry has addressed all five of the college goals for liberal learning. As a course, I believe we have discussed as many diverse topics as possible and related them to the topic of the course, neurochemistry. We learned about and discussed everything from Alzheimer’s Disease to medical marijuana, while also addressing each topic from our unique perspectives. Within the course, we had psychology students, neuroscience students, chemistry students, biology students, pre-pharmacy students, pre-medical students, musicians, athletes, student leaders, and a whole gambit of personal experiences to draw from.
As a capstone to my Neuroscience major at Concordia College, Neurochemistry has addressed all five of the college goals for liberal learning. As a course, I believe we have discussed as many diverse topics as possible and related them to the topic of the course, neurochemistry. We learned about and discussed everything from Alzheimer’s Disease to medical marijuana, while also addressing each topic from our unique perspectives. Within the course, we had psychology students, neuroscience students, chemistry students, biology students, pre-pharmacy students, pre-medical students, musicians, athletes, student leaders, and a whole gambit of personal experiences to draw from.  Instill a love of learning.
Instill a love of learning.  The fifth and final goal of liberal learning, “encourage responsible participation in the world,” came through in not only our class discussions, but our community action projects. As an aspect of the course, we worked in groups to address an issue within the community related to mental illness, PTSD, Alzheimer’s Disease, or Autism Spectrum Disorder. The community action project that the group I was part of addressed the stigma of mental health on campus. At Concordia, there is a pressure to identify as a “Happy Cobber.” The phrase is well-known among students and distressful to many. Additionally, the college Instagram account at the beginning of the year posted a photo of Kernel, the school mascot, leaning against the words, “NO BAD DAYS.” Within a few hours, the post was deleted due to the backlash of students who thought it was wrong for the college to insinuate that students cannot have bad days or that the statement was invalidating the experience of many Cobbers with mental health conditions. Knowing these things, the goal of our project was to raise awareness of the realness of mental health on campus through a social media takeover on Concordia’s official Instagram page. We addressed the “Happy Cobber” and proposed the “Real Cobber.” I recorded and edited videos of students, faculty, and community resources discussing the stigma of mental health on campus, the resources available to students on and off campus, and the message that participants had for individuals struggling with mental health. All of these videos were posted on the college Instagram story, and for the first time, a discussion of mental health was coming from the official Concordia social media profile. Likewise, we tabled during Mental Health Awareness week as a group to raise advocate against the stigma of mental health, raise awareness of the neurochemistry behind mental illness, and provide information regarding on and off campus resources. Due to its impact and originality, this community action project was likely my favorite way that I have became responsibly engaged in the world for a class project during my time at Concordia.
The fifth and final goal of liberal learning, “encourage responsible participation in the world,” came through in not only our class discussions, but our community action projects. As an aspect of the course, we worked in groups to address an issue within the community related to mental illness, PTSD, Alzheimer’s Disease, or Autism Spectrum Disorder. The community action project that the group I was part of addressed the stigma of mental health on campus. At Concordia, there is a pressure to identify as a “Happy Cobber.” The phrase is well-known among students and distressful to many. Additionally, the college Instagram account at the beginning of the year posted a photo of Kernel, the school mascot, leaning against the words, “NO BAD DAYS.” Within a few hours, the post was deleted due to the backlash of students who thought it was wrong for the college to insinuate that students cannot have bad days or that the statement was invalidating the experience of many Cobbers with mental health conditions. Knowing these things, the goal of our project was to raise awareness of the realness of mental health on campus through a social media takeover on Concordia’s official Instagram page. We addressed the “Happy Cobber” and proposed the “Real Cobber.” I recorded and edited videos of students, faculty, and community resources discussing the stigma of mental health on campus, the resources available to students on and off campus, and the message that participants had for individuals struggling with mental health. All of these videos were posted on the college Instagram story, and for the first time, a discussion of mental health was coming from the official Concordia social media profile. Likewise, we tabled during Mental Health Awareness week as a group to raise advocate against the stigma of mental health, raise awareness of the neurochemistry behind mental illness, and provide information regarding on and off campus resources. Due to its impact and originality, this community action project was likely my favorite way that I have became responsibly engaged in the world for a class project during my time at Concordia.

 Discussing obesity becomes difficult when considering every side of the “argument.” Between social advocacy to the neurochemistry of weight, many perspectives have to be considered. Body positivity has been a growing concept within society over the past decade, and I would argue that this is a good thing. Often, body image is a socially derived concept and is not just the individual’s physical appearance, but how the individual perceives themselves. In many cases, due to societal pressures, people perceive themselves as heavier than they actually are. These perceptions may lead to mental health concerns, primarily the development of eating disorders. Reward related brain areas are involved in eating disorders. Specifically, in bulimia nervosa, bingeing on foods that taste good leads to the release of dopamine, while the purging of food reduces the signal or effectiveness of acetylcholine. Acetylcholine signaling normally indicates when an individual is full or nutritionally satisfied. In anorexia nervosa, research has suggested that food intake following periods of starvation increases the amount and effect of dopamine within the reward pathway. In cases of anorexia, individuals tend to have a variant of the 5HT2A serotonin receptor responsible for releasing too much serotonin during non-starvation periods. Researchers hypothesize that an individual with anorexia may feel better during a starvation period because it reduces the amount of serotonin. In contrast, individuals with bulimia and binge eating disorder experience lower-than-normal levels of serotonin. In these cases, the individual tends to excessively eat in order to increase serotonin and decrease depressed mood.
Discussing obesity becomes difficult when considering every side of the “argument.” Between social advocacy to the neurochemistry of weight, many perspectives have to be considered. Body positivity has been a growing concept within society over the past decade, and I would argue that this is a good thing. Often, body image is a socially derived concept and is not just the individual’s physical appearance, but how the individual perceives themselves. In many cases, due to societal pressures, people perceive themselves as heavier than they actually are. These perceptions may lead to mental health concerns, primarily the development of eating disorders. Reward related brain areas are involved in eating disorders. Specifically, in bulimia nervosa, bingeing on foods that taste good leads to the release of dopamine, while the purging of food reduces the signal or effectiveness of acetylcholine. Acetylcholine signaling normally indicates when an individual is full or nutritionally satisfied. In anorexia nervosa, research has suggested that food intake following periods of starvation increases the amount and effect of dopamine within the reward pathway. In cases of anorexia, individuals tend to have a variant of the 5HT2A serotonin receptor responsible for releasing too much serotonin during non-starvation periods. Researchers hypothesize that an individual with anorexia may feel better during a starvation period because it reduces the amount of serotonin. In contrast, individuals with bulimia and binge eating disorder experience lower-than-normal levels of serotonin. In these cases, the individual tends to excessively eat in order to increase serotonin and decrease depressed mood.
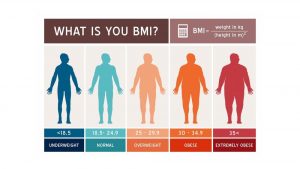
 Although we understand the issue of obesity from a medical perspective, the social aspect must also be considered. In many cases, individuals who are deemed overweight by physicians do not receive proper medical care. Likewise, individuals of a higher BMI are less likely to seek medical advice, typically due to stigma and the fear of being judged. As someone who has worked in a hospital, I have seen these tendencies first-hand. I have heard nurses comment about a patient’s weight in a derogatory manner, often blaming the patient for their health concerns. As many of us prepare to enter the medical field in some way, we need to consider all aspects of someone’s condition, not just their weight. People are more than their BMI, and typically, weight is a genetically-determined factor within the whole scheme of an individual’s wellness.
Although we understand the issue of obesity from a medical perspective, the social aspect must also be considered. In many cases, individuals who are deemed overweight by physicians do not receive proper medical care. Likewise, individuals of a higher BMI are less likely to seek medical advice, typically due to stigma and the fear of being judged. As someone who has worked in a hospital, I have seen these tendencies first-hand. I have heard nurses comment about a patient’s weight in a derogatory manner, often blaming the patient for their health concerns. As many of us prepare to enter the medical field in some way, we need to consider all aspects of someone’s condition, not just their weight. People are more than their BMI, and typically, weight is a genetically-determined factor within the whole scheme of an individual’s wellness.