

First of all, let’s establish that schizophrenia is a mental illness. You probably knew this already, but if I had asked you to name the first three mental illnesses that came to your mind, what would they have been? Anxiety? Depression? And maybe Alzheimer’s or PTSD? The point is that some mental illnesses have become topics of discussion more so than others, leading to a better understanding of them by the general public. However, mental health awareness is important for any type of disorder, especially when almost half of all US adults will experience a mental illness at some point in their lives.
On that note, here are 10 things you should know about schizophrenia:
1. Schizophrenia affects how a person thinks, feels, behaves, and perceives reality: Many people misunderstand this disorder because they believe having schizophrenia means having multiple personalities. This is false. The word schizophrenia comes from a Greek word meaning “split mind”, which refers to the mind being split from reality or from the rest of the world. It does not mean that the mind itself is split into different personalities. That is a separate disorder called Dissociative Identity Disorder (formerly Multiple Personality Disorder).
2. It has been estimated that about 40% of people with schizophrenia do not receive treatment on a yearly basis: In the US, approximately 1% of adults are affected by schizophrenia at any given time. This equates to over 2 million people and forty percent of that is 800,000 humans who are not being treated.
3. Five subtypes of the disorder exist. They are: Paranoid Schizophrenia, Schizoaffective Disorder, Catatonic Schizophrenia, Disorganized Schizophrenia and Residual Schizophrenia. For more information on these subtypes click here.
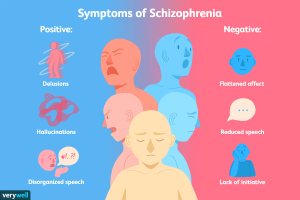
4. Schizophrenia has positive symptom: Positive symptoms are the presence of behaviors generally not seen in healthy individuals. These can include hallucinations, delusions, thought disorders (unusual or dysfunctional thinking), or movement disorders (agitated body movements).
5. Schizophrenia has negative symptoms: Negative symptoms are the absence of behaviors and emotions usually present in healthy individuals. These include so called flat affect (less facial and/or vocal expression of emotion), generally reduced feelings of pleasure, less speaking, and more difficulty joining and continuing to participate in activities.
6. Schizophrenia has cognitive symptoms: Cognitive symptoms have a higher variability among patients, where some experience them quite subtly and others more severely. They can include decreased executive functioning (the ability to understand and use information), reduced focus or attention, and problems with working memory (being able to use information after just learning it).
7. The first expression of schizophrenia usually occurs around someone’s late adolescence or their 20s. This video briefly describes the story of someone who was diagnosed with the illness at 29:
8. The idea that people suffering from schizophrenia are violent is a myth: Oftentimes movies, TV and other pop culture portray people with mental illnesses as criminals, which has led to the false idea that people with schizophrenia are dangerous. They actually tend to prefer to be alone, and of the few people who have committed violent crimes, only about 23% of them were related to schizophrenic symptoms.
9. There is no cure, but treatments do exist: These focus on eliminating the symptoms and are usually in the form of medication or therapy. Antipsychotic medications tend to be in the form of pills or liquids, and some types can be given as injections once or twice a month. Side effects usually diminish or disappear within a few days. Psychosocial treatments are a strong supplemental option, and those patients who follow through with them have demonstrated a decreased likelihood to relapse or be hospitalized because they learn and can use coping skills to address every day challenges.
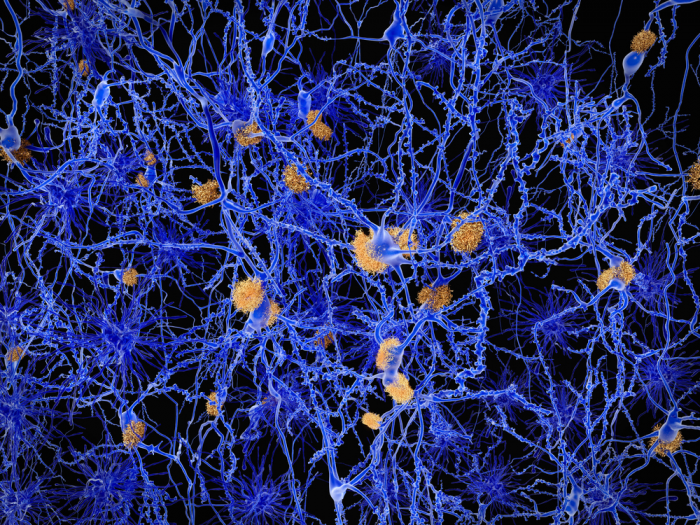
10. The cause is unknown, but different factors can influence its development: To better understand the risk factors described below, we first discuss the Wnt signaling pathway in the brain: In its inactive state, Wnt ligands do not bind to their receptors, allowing the existence of a destruction complex that contains GSK3. GSK3 in return phosphorylates β-catenin, but also leads to its degradation, meaning no gene transcription occurs. However, when Wnt ligands do bind to their receptors, the destruction complexes are dissociated because parts of them (APC and Dvl) are recruited to the membrane. This allows for more β-catenin in the cytoplasm, which can be translocated to the cell nucleus, enhancing TCF/LEF mediated gene transcription.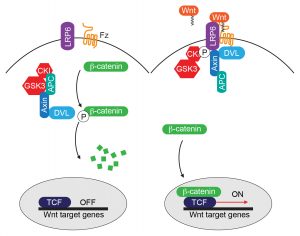
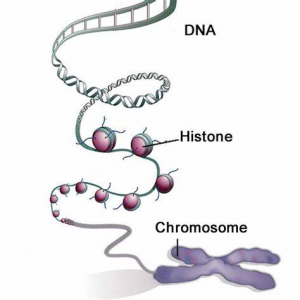
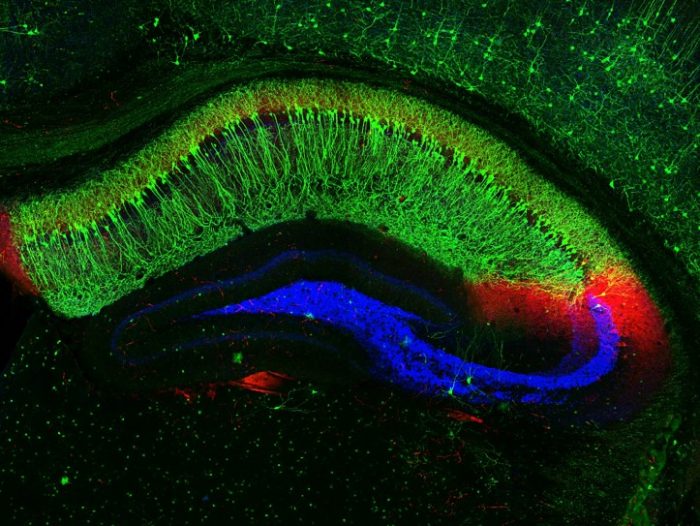
Risk factors: Due to the fact that schizophrenia can sometimes run in families, scientists know there must be a genetic aspect for the development of schizophrenia, though environmental factors are most likely to be very influential as well. It is believed that multiple genes may increase the risk for developing the disorder, but that no single gene actually causes schizophrenia. Environmentally, factors such as exposure to viruses, malnutrition before birth, problems during birth, or psychosocial factors are considered necessary for the development of schizophrenia. All of the above may in the end be related to changes in brain chemistry and structure.
Connection to Wnt signaling: A number of steps in the Wnt signaling pathway can go wrong or be affected by molecules outside of the pathway. Too much dopamine (a neurotransmitter, which brain cells use to communicate) can increase the activity of GSK3, later leading to a decrease in gene transcription. Not enough glutamate (another neurotransmitter) can lead to a similar effect. What exactly leads to these phenomena still remains unclear, but this article provides an in depth look at Wnt signaling.

 Low levels of GABA have been linked to anxiety and PTSD. Researchers allowed rats to exercise and found that exercise results in an increased production of GABA. When these rats were then introduced to a stressful event, they relaxed much quicker than the rats that didn’t exercise.
Low levels of GABA have been linked to anxiety and PTSD. Researchers allowed rats to exercise and found that exercise results in an increased production of GABA. When these rats were then introduced to a stressful event, they relaxed much quicker than the rats that didn’t exercise. Background
Background





 The years were hard and at times but I would not trade it for the world. I have made many friends, learned astronomical amounts of information that sometimes felt insignificant, paved the way for the future students, became responsibly engaged in my community, and ultimately grew as a person. I am proud to be where I am today because of Concordia, and this class did a great job of highlighting that. So I say thank you Concordia, thank you to all the faculty who have taught me not only textbook materials but life skills. Thank you to all the people that supported me, to all the friends I have made and to those who have been essential in shaping who I am today. Thank you for your liberal learning practices and allowing me to grow, not only as a student but within the world, for my critical thinking and reasoning skills, and for making me a better and more informed person. There is nothing left to say but thank you. As of now, the light at the end of the tunnel is visible and though I do not know what is on the other side, I walk to it gladly, awaiting the new adventures to be found. When I walk across that stage this May I will be forever proud to call Concordia my alma mater.
The years were hard and at times but I would not trade it for the world. I have made many friends, learned astronomical amounts of information that sometimes felt insignificant, paved the way for the future students, became responsibly engaged in my community, and ultimately grew as a person. I am proud to be where I am today because of Concordia, and this class did a great job of highlighting that. So I say thank you Concordia, thank you to all the faculty who have taught me not only textbook materials but life skills. Thank you to all the people that supported me, to all the friends I have made and to those who have been essential in shaping who I am today. Thank you for your liberal learning practices and allowing me to grow, not only as a student but within the world, for my critical thinking and reasoning skills, and for making me a better and more informed person. There is nothing left to say but thank you. As of now, the light at the end of the tunnel is visible and though I do not know what is on the other side, I walk to it gladly, awaiting the new adventures to be found. When I walk across that stage this May I will be forever proud to call Concordia my alma mater.
 Image Source: https://image.tmdb.org/t/p/w1280/ApuCppLxFVm8B1NRecs0L8ej4Tj.jpg
meme: by me
Image Source: https://image.tmdb.org/t/p/w1280/ApuCppLxFVm8B1NRecs0L8ej4Tj.jpg
meme: by me