“I use CBD oil with my dog to calm his separation anxiety when I’m gone or when we travel.”
“I use CBD oil for muscle pain when my neck is sore instead of ibuprofen.”
“I know of many pet owners that give CBD in some form to their pets to help with arthritis.”
These are just a few quotes from people in my life who have had positive outcomes from using CBD oil as a therapeutic technique for various pain, illness, etc. CBD in many forms, but especially oil, has become very popular as a therapeutic way of treating a variety of aches, pains, diseases, and more.
What’s the difference?
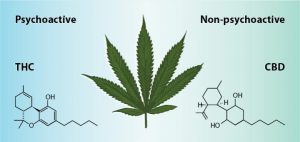
CBD (cannabidiol) and THC (tetrahydrocannabinol) are the same compound besides one simple atom. But that one atom has a big impact on the difference between these two compounds.
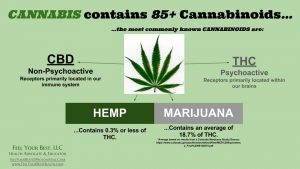
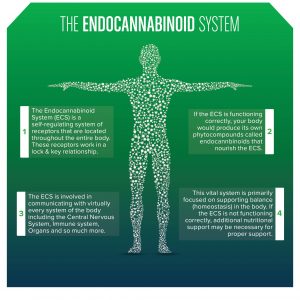
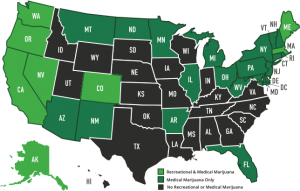
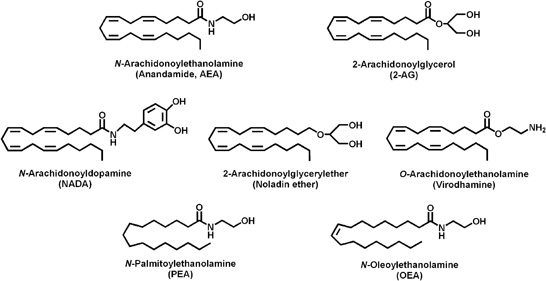
As shown above, there a tons of cannabinoids in cannabis, but CBD and THC are the most prominent. These cannabinoids interact with the endocannabinoid System (ECS) which basically is a big network of receptors that interact with cannabinoids to maintain vital functions throughout our body (find out more about cannabinoids here https://medium.com/cbd-origin/cbd-vs-thc-the-difference-explained-b3cfc1da52f0). The difference between the two cannabinoids is how it binds to certain receptors in the ECS. These bindings can produce different effects like a psychoactive effect on your brain or not. Another difference between the two is the legality. Hemp-derived CBD is legal in all 50 states, but ‘marijuana’-derived CBD is not legal federally. So if you were to go to a health product store in your town, you will be buying CBD oil from hemp. This is not only because of legality but also because the hemp plant has far more CBD than marijuana plants, which have much more THC.
Possible effects of CBD
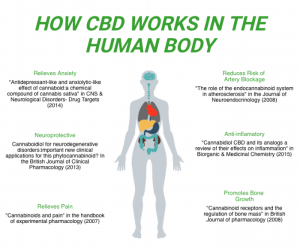
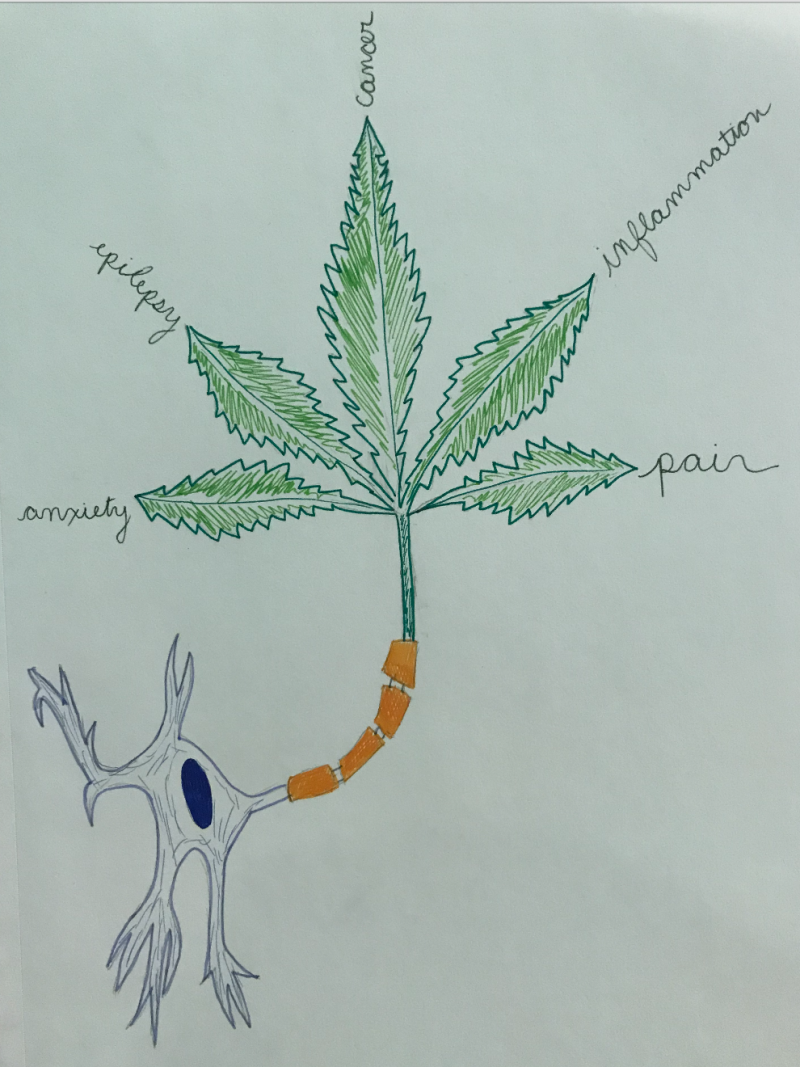
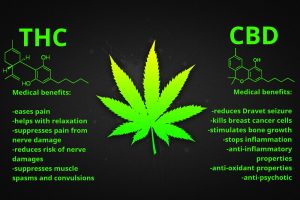
For the purpose of discussing CBD, we can use CBD oil as the therapy of choice. For years, many research articles have shown how cannabinoids can help ease anxiety and pain through many ways. Below are some benefits of CBD oil.
- Reduce anxiety/depressive symptoms
- Alleviate cancer-related symptoms
- Relieve pain
- Benefit heart health
- May reduce acne
- Have neuropcrotecive properties (benefit neurological disorder symptoms like spasms, seizures, denigration of neurons)
You can read more on the scientific research behind each of these benefits here: https://www.healthline.com/nutrition/cbd-oil-benefits#section5
As discussed above, CBD oil has several great benefits to it’s use. As with any pharmacological drug that may be prescribed by a physician, the outcomes and side effects will vary from person to person. There can be many factors that impact CBD oil’s effect such as other prescription drugs or over-the-counter medications you take, the dosage and frequency you use CBD oil, and how severe your symptoms of pain. For these reasons and more, it is important to remember that CBD oil will most likely work differently for each person who tries it.
I believe that CBD oil is a great alternative medicine to other drugs. It can be used for such a wide variety of pain and illnesses that when possible, CBD should be studied more in order to further our knowledge of how therapeutic this drug can be.
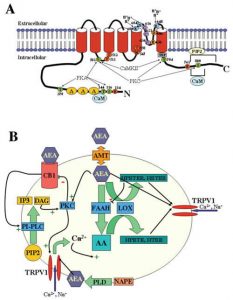
 CB1 receptors are typically found in the brain and can influence behavior, memory, cognition and movement. These receptors modulate adenylyl cyclase and therefore the the intracellular cAMP levels which regulates regulates protein kinase A (PKA) phosphorylation. This causes changes in the cellular activity. The CB2 receptors are predominantly associated with immune cells and modulating the immune system. Activation of these receptors can promote neuro-protection
CB1 receptors are typically found in the brain and can influence behavior, memory, cognition and movement. These receptors modulate adenylyl cyclase and therefore the the intracellular cAMP levels which regulates regulates protein kinase A (PKA) phosphorylation. This causes changes in the cellular activity. The CB2 receptors are predominantly associated with immune cells and modulating the immune system. Activation of these receptors can promote neuro-protection
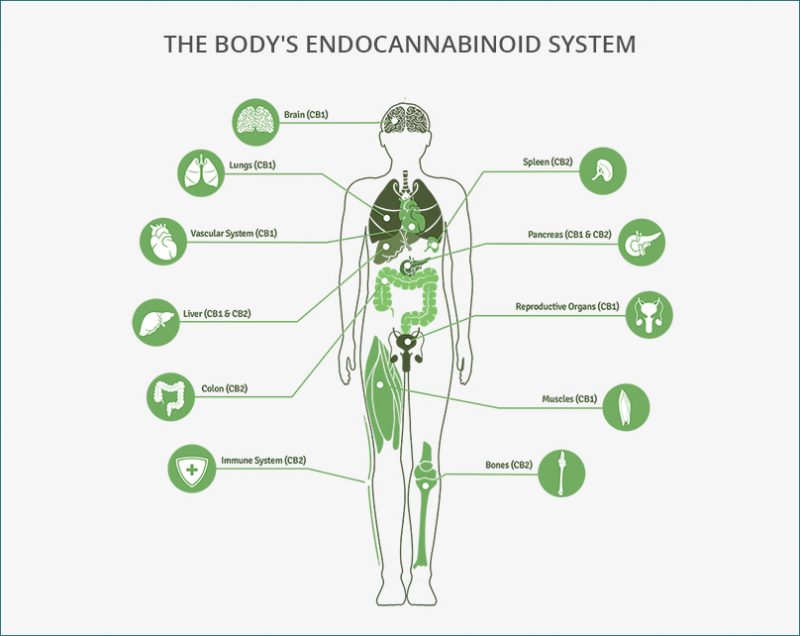
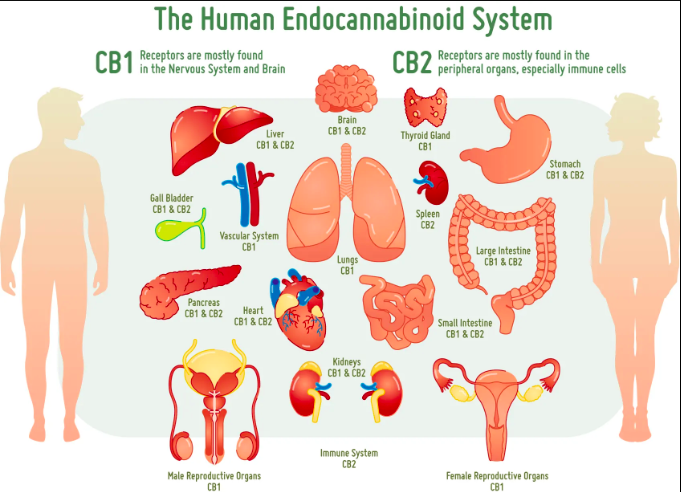
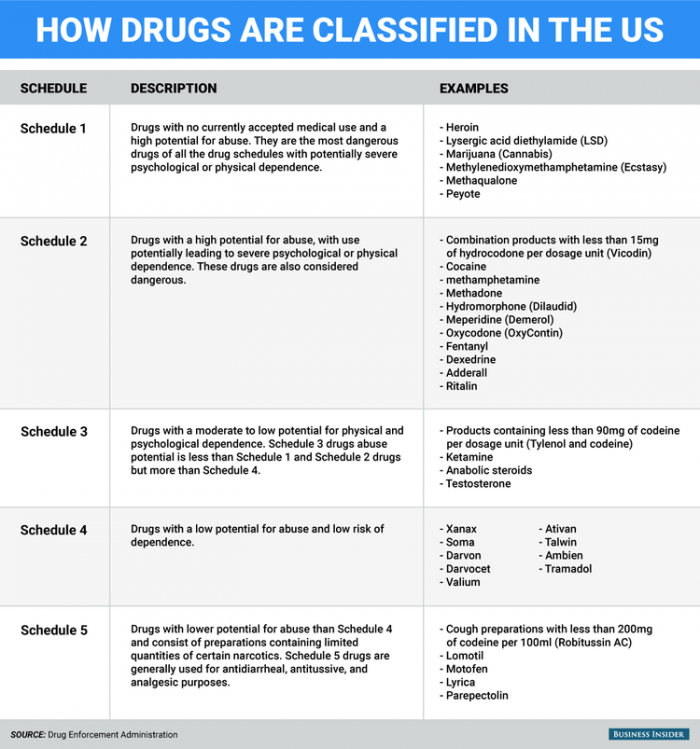
 Due to its classification as a schedule one drug, not enough research has been done on cannabis. Although we don’t understand everything about cannabis, we do know that the endocannabinoid system is present across the human body, not just in the brain. This is one reason why medical marijuana use can aid in pain control, over/under eating, and cancer.
Due to its classification as a schedule one drug, not enough research has been done on cannabis. Although we don’t understand everything about cannabis, we do know that the endocannabinoid system is present across the human body, not just in the brain. This is one reason why medical marijuana use can aid in pain control, over/under eating, and cancer.