In the past few years, there has been controversy surrounding concussions in the National Football League (NFL). It all began to snowball in 2002, where Dr. Bennet Omalu identified chronic traumatic encephalopathy (CTE) in the brain of Mike Webster, 50, a former Pittsburg Steeler whom committed suicide. Webster being the first case of CTE found in American football players.

CTE is a very scary degenerative brain disease most prevalent in athletes, military veterans, and others with a history of repeated brain trauma. CTE is characterized by Tau protein aggregating and killing brain cells; the same protein plays a role in Alzheimer’s disease. Symptoms of CTE include memory loss, confusion, decreased cognitive functioning, behavioral changes, impaired judgement, and eventually progressive dementia. As with any degenerative diseases, symptoms worsen over time.
CTE is caused by many repeated blows to the head, which have been nearly unavoidable in football. These hits, combined with the magnitude of force behind them are a significant cause of concern for the immediate and future safety of the players. However, it was not until March 2016 where the NFL openly admitted to a connection between football and CTE. This statement was only after copious amounts of irrefutable research and film was presented to the NFL.
Later in 2016, the NFL and NFL Player’s Association implemented a new policy to enforce a concussion protocol, and a similar concern was echoed by Commissioner Goodell to increase the safety of the game specifically by attempting to reduce the number of head injuries sustained as well as offer better protocols for those who have suffered an injury.
Such actions involved having a neurologist on the field to determine if a player has suffered a concussion after a significant blow to the head. Other actions include making certain blocks and hits involving specific head to head contact illegal. Particular care was placed on plays during kickoffs, which have proven to be the most dangerous plays, which makes sense because you have 300 lb men sprinting as fast as they can 70 yards and hitting others as hard as possible making a very dangerous situation for both the receiving and the kicking team.

In the 2016-17 season, the impact of these new restrictions was lackluster, there were very few penalties called by the referees. Therefore, when there was a call made correctly as implicated by the new rules, many players, coaches, and fans alike would become very frustrated. This inconsistency of calling opened the NFL up to criticism by many.
Moreover, a study published in July 2017 identified CTE in 99% of deceased NFL players’ brains. The players donated their brains for the study, so the study is not 100% reflective of the NFL as a whole, but the sheer magnitude of 99% (110/111 players) should be met with a striking concern.
Moving forward in the 17-18 and 18-19 season, referees have become much more consistent and aware to which plays are illegal and deserve to be penalized. Many fans are still upset about the rules and a common sentiment being, “it changes the integrity of the game.” This is inherently true, but as the players adjust to the tighter hitting restrictions, there will be fewer interruptions due to appropriately called penalties, and the game will continue on.

Yes, the game will never be the same. But, do we really want a game where the players are receiving head injury after head injury causing them to have severe neurological issues? The safety and well-being of the players should reign over the “big hit” mentality. There will undoubtedly still be big hits, just not hits by a head or to a head.
https://www.cnn.com/2013/08/30/us/nfl-concussions-fast-facts/index.html
http://www.espn.com/nfl/story/_/id/24743994/really-changed-nfl-call-action-concussions


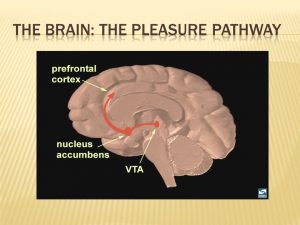
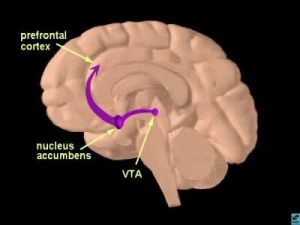 The human brain is capable of many complex memories and emotions all driven by chemical interactions and signaling in distinct brain regions. In response to experiences like eating food, sleeping, or having sex a portion of the brain called the reward pathway is activated. This pathway creates lasting memories connecting certain activities with the feeling of reward and encouraging repetition of the behaviors. Activation of this pathway takes place in the ventral tegmental area (VTA) which projects to the nucleus accumbens (NAc), with signals propagated by the release of the neurotransmitter dopamine. Dopamine creates the feelings of euphoria and energy and function to remind our brains to do things that help us survive.
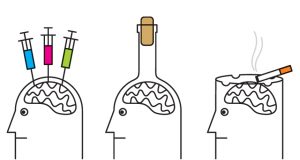
The human brain is capable of many complex memories and emotions all driven by chemical interactions and signaling in distinct brain regions. In response to experiences like eating food, sleeping, or having sex a portion of the brain called the reward pathway is activated. This pathway creates lasting memories connecting certain activities with the feeling of reward and encouraging repetition of the behaviors. Activation of this pathway takes place in the ventral tegmental area (VTA) which projects to the nucleus accumbens (NAc), with signals propagated by the release of the neurotransmitter dopamine. Dopamine creates the feelings of euphoria and energy and function to remind our brains to do things that help us survive. However, when addictive drugs are involved in this brain circuitry and dopamine levels are unnaturally raised the reward pathway is overthrown. A large euphoric high along with the connection of drug using behaviors with the reward leads to what we know as addiction and drug seeking behaviors. Addictive drugs act in different ways in the brain, but all function to make more dopamine available to activate the neurons in the NAc and signaling to the frontal cortex.
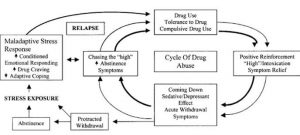
However, when addictive drugs are involved in this brain circuitry and dopamine levels are unnaturally raised the reward pathway is overthrown. A large euphoric high along with the connection of drug using behaviors with the reward leads to what we know as addiction and drug seeking behaviors. Addictive drugs act in different ways in the brain, but all function to make more dopamine available to activate the neurons in the NAc and signaling to the frontal cortex. The stress pathway can add to the dopamine levels in the reward pathway and compound drug-seeking behaviors in addiction. The release of dopamine driven by glucocorticoid hormones functions to increase the euphoric sense and desire to return to the behavior triggering the reaction. In an experiment done on rats addicted to cocaine, after being given a small amount of cocaine as a trigger, rats with excess stress hormones or an external stressor showed more signs of relapse than those that did not have increased stress levels.
The stress pathway can add to the dopamine levels in the reward pathway and compound drug-seeking behaviors in addiction. The release of dopamine driven by glucocorticoid hormones functions to increase the euphoric sense and desire to return to the behavior triggering the reaction. In an experiment done on rats addicted to cocaine, after being given a small amount of cocaine as a trigger, rats with excess stress hormones or an external stressor showed more signs of relapse than those that did not have increased stress levels.




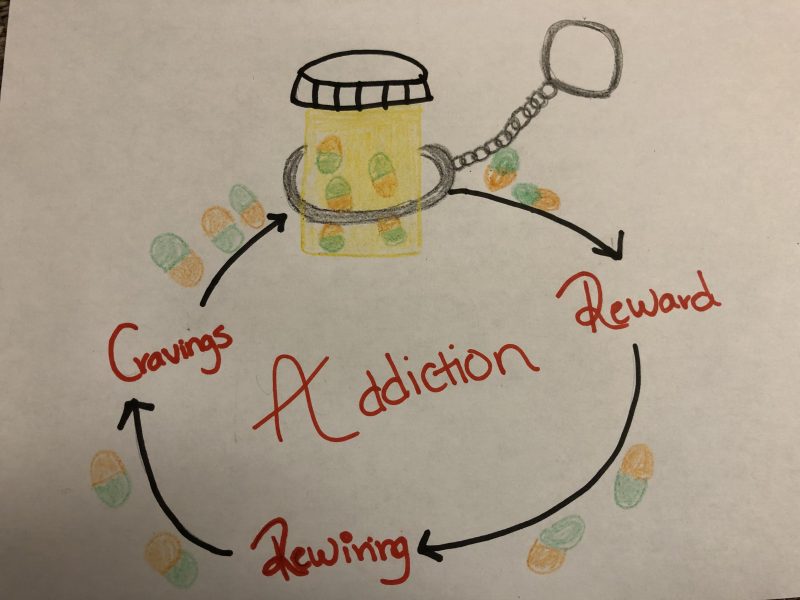

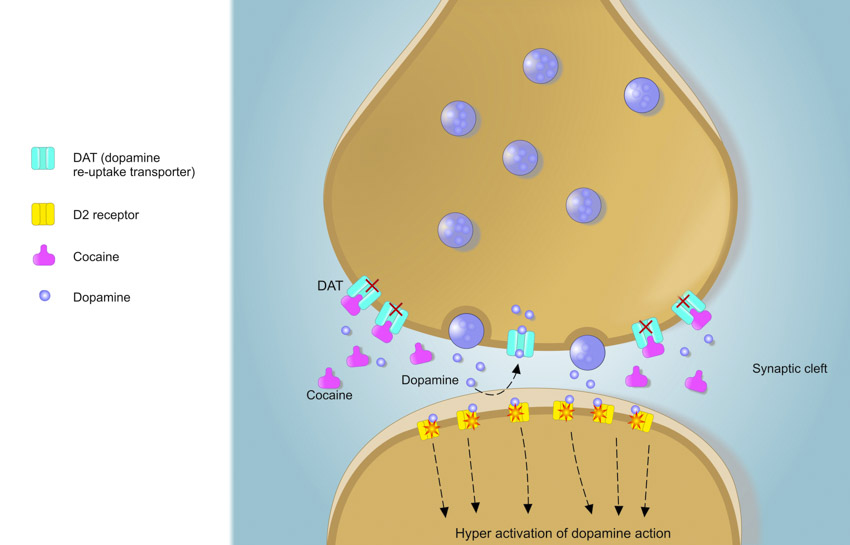
 dopamine in the frontal cortex, the nucleus accumbens, and ventral tegmental area increase, and give the person a sense of euphoria. Drugs of abuse have a way of making this euphoria or “high” last for a prolonged time. Cocaine, for example, blocks dopamine re-uptake thus causing the reward to stay in a person’s system for longer. When a drug of abuse is taken for a long time the amount of dopamine decreases, and the “high” decreases. The individual will begin to crave their drug of choice, and if they are unable to gain access to that drug they will begin to experience withdrawal. To satisfy their cravings, due to the rewiring in the brain, a person will take more of their drug of abuse in order to experience a high, and without even noticing the person has become ADDICTED.
dopamine in the frontal cortex, the nucleus accumbens, and ventral tegmental area increase, and give the person a sense of euphoria. Drugs of abuse have a way of making this euphoria or “high” last for a prolonged time. Cocaine, for example, blocks dopamine re-uptake thus causing the reward to stay in a person’s system for longer. When a drug of abuse is taken for a long time the amount of dopamine decreases, and the “high” decreases. The individual will begin to crave their drug of choice, and if they are unable to gain access to that drug they will begin to experience withdrawal. To satisfy their cravings, due to the rewiring in the brain, a person will take more of their drug of abuse in order to experience a high, and without even noticing the person has become ADDICTED.

 Addiction occurs when a person is physically and mentally dependent on a specific substance. Most the time, the substance is a drug. Drug addiction has always been depicted as a choice. From the outside, it has always seemed that getting rid of an addiction should be as easy as stopping the intake of the drug. However, research into drug addiction has shown that it is actually a disease of the brain. Drugs alter a very important pathway in the brain called the reward pathway by blocking the reuptake of signaling molecules, thus increasing reward signaling. Altering this pathway creates long lasting changes in the addict’s brain, which makes it very difficult for addict’s to stop their drug intake.
Addiction occurs when a person is physically and mentally dependent on a specific substance. Most the time, the substance is a drug. Drug addiction has always been depicted as a choice. From the outside, it has always seemed that getting rid of an addiction should be as easy as stopping the intake of the drug. However, research into drug addiction has shown that it is actually a disease of the brain. Drugs alter a very important pathway in the brain called the reward pathway by blocking the reuptake of signaling molecules, thus increasing reward signaling. Altering this pathway creates long lasting changes in the addict’s brain, which makes it very difficult for addict’s to stop their drug intake. Dopamine binds to dopamine receptors in the synaptic space, which stimulates the neuron, creating the pleasurable sensation. Once the action potential that releases the dopamine is over, dopamine is removed from the synaptic space back into the transmitting neuron via a dopamine transporter. This ensures that the reward is cognitively linked to the stimulus.
Dopamine binds to dopamine receptors in the synaptic space, which stimulates the neuron, creating the pleasurable sensation. Once the action potential that releases the dopamine is over, dopamine is removed from the synaptic space back into the transmitting neuron via a dopamine transporter. This ensures that the reward is cognitively linked to the stimulus.