
Starting a family is a wonderful adventure for many couples. Everything is expected to go smoothly, and more often than not it does, with the exception of a few hurdles along the way. In some cases however, the obstacles can cause complications with development or potentially permanent changes after birth.
Pregnancy is a period of time in which a mother must be exceptionally cautious and aware of her state of well-being. Certain environmental factors and health problems have the possibility of triggering the development of autism in children who are already genetically predisposed to the condition.
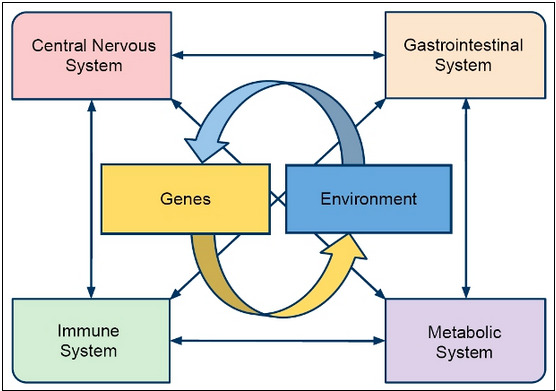
Factors involved with autism
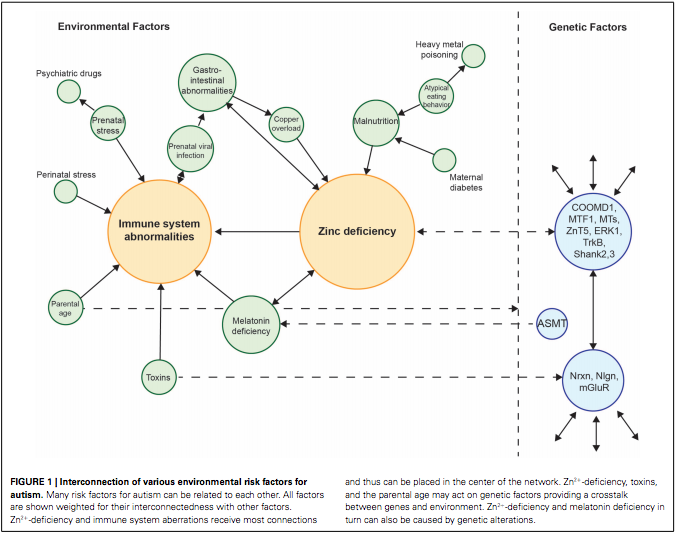
The statistics show that autism is becoming more prevalent in children today. The levels are rising, but why? Researchers have been gathering data, and the results show that there are two common factors linked with the cause of autism. These factors are maternal zinc deficiency and maternal immune dysfunction. Both are attributed heavily to environmental factors, such as diet, parental age, maternal exposure to toxins, melatonin deficiency, prenatal infection, prenatal stress, copper overload, and GI abnormalities.
Zinc
All of these factors have the potential to influence zinc levels and/or immune function. The zinc deficiency is harmful because it causes neuropsychological symptoms, behavioral problems and learning and memory impairments. It can also lead to an excessive amount of the excitatory neurotransmitter, glutamate, which can cause seizures. Zinc is a vital element that it is found in every tissue of the body and is needed for enzymes to function properly. Pregnant women should be tested to ensure their zinc levels are sufficient, and thereby eliminate a risk factor for the development of autism in their child.
Immune System
The increased production of cytokines (cells involved in the immune response) resulting from immune dysfunction is dangerous because it causes inflammation, which can lead to excessive signaling and overgrowth in the brain. The cytokines have detrimental effects on neuronal plasticity, function, and viability. The immune response can be activated due to stress or illness experienced by the mother. The zinc deficiency, GI problems, toxin exposure and parental age also play a role in triggering the immune system.
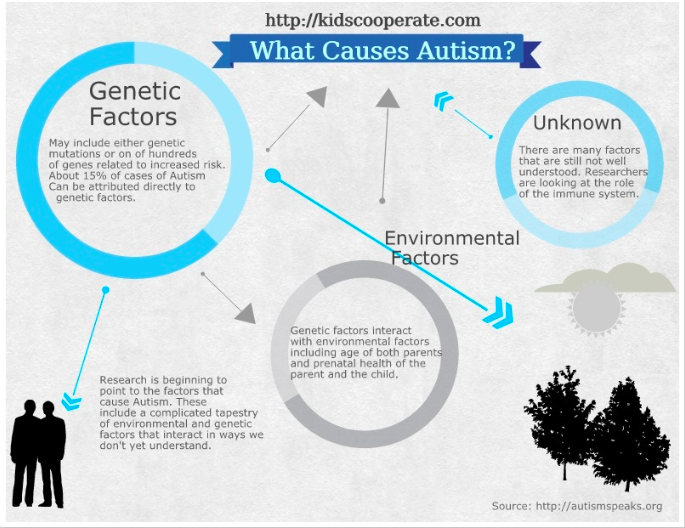
Given the information described above, it seems as though autism could easily develop at the slightest health disturbance. The important fact to keep in mind is that a combination of both genetic and environmental components leads to the occurrence of autism. Considering the variety of factors that influence neuronal development, it is very challenging to pin point the cause of autism. This makes it rather difficult to stop the development of autism. The best prevention is for a mother to look out for her health during pregnancy by avoiding illness, managing stress, eating healthy, and steering clear of toxic substances.

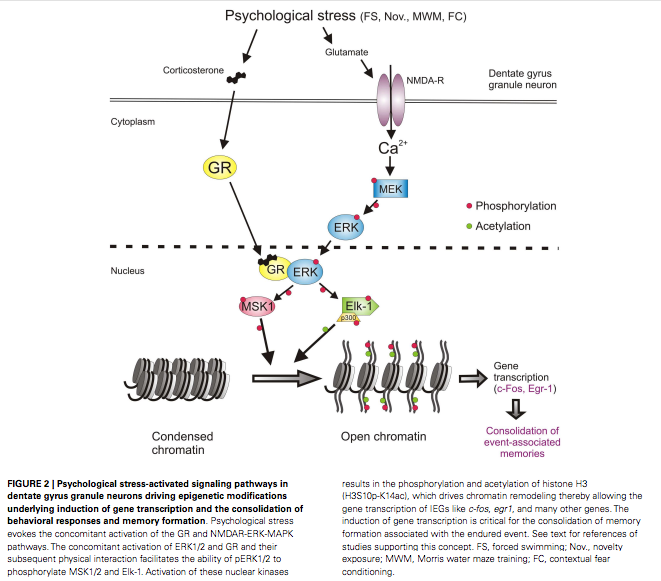
Figure 2. Excessive excitation occurring within the brain of a child with autism
For more information on environmental factors in autism, please visit
https://moodle.cord.edu/pluginfile.php/625310/mod_resource/content/1/autism%20and%20environ.pdf
Autism: Factors Understood, Cause Not Yet Ascertained














{kind=link}
{kind=link}
{kind=link}