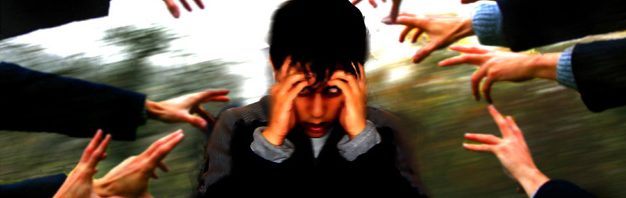
The Treatment Advocacy Center states that 1.1% of the world population is affected by schizophrenia and it is estimated that 40% of people with schizophrenia go untreated. Some symptoms of schizophrenia include delusions and hallucinations, changes in emotions movements and behavior, alterations of senses, an altered sense of self and the inability to sort and interpret what is going on.
There are numerous changes in the brain with schizophrenia, but not one specific condition that can be measured for diagnosis. The disease must be diagnosed by a measure of its symptoms. There are high functioning patients with schizophrenia who are able to carry on a mostly normal life while others must be hospitalized.
Schizophrenia is a brain development disorder, so it is difficult to prevent because we don’t see the effects until it has already progressed. There are studies that show that infections during pregnancy may disrupt fetal brain development which increases the risk of schizophrenia.
In the article we talked about this week found the main problem with schizophrenia is not enough Wnt signaling and overactive dopamine in the brain. The combination of these two cause increased phosphorylation of β-catenin. When β-catenin is phosphorylated it has no positive effects on the brain.
Wnt proteins are produced by wnt genes in the body and are used all over the body, many of the proteins are organ or tissue specific. Evidence of increased dopamine production as well as increased ability for dopamine to interact with its receptor have been a part of discovering dopamine’s role in schizophrenia.
β-cateinin is used across the body for cell-cell adhesion and gene expression. In schizophrenia there is not enough β-catenin, but many cancers are associated with the over expression of β-catenin.
The best thing we can do to help with the research in Schizophrenia is become informed. The more we talk about it, the more aware we will be about the symptoms, prevention, and treatments.