
Cannabis: Reaching a New “High”
We humans have a close relationship with the kingdom of plants. Produce graces our table each night at dinner with a cornucopia of colors and flavors. Age-old oaks stand tall in their glory providing shade over our parks and dropping leaves for our children to pile. And who can forget the marvelous flowers that fill the air with delicious scents? But there is a plant the strikes controversy in the general public. Some give it praise for its effects while others shun it for the same reason. This plant is cannabis.
Cannabis is notoriously associated with the production of marijuana, a drug that causes a slew of physical and psychoactive effects. But it is not the whole cannabis plant that causes these effects. Within the plant is a chemical called Δ9-tetrahydrocannabinol which is much more commonly known as THC. THC is the active ingredient in marijuana that is responsible for the variety of effects on the body. So how exactly does this happen?
When THC is ingested, it travels through the cells of the body searching for two specific proteins that will receive the THC with warm welcome. These proteins are called CB1 and CB2 and are specialized types of proteins called receptors. While many proteins in the body are used to process the nutrients we eat or to stimulate growth of our muscles, these receptors are used as our body’s communication network.
Imagine that you have just received a text message from your spouse that reads “Can you stop and pick up milk on your way home from work?” Assuming that you don’t reply “I’m pretty busy, can you do it instead?” this text would signal a response from you that would cause you to stop at the grocery store and coincidentally purchase a gallon of milk. This same situation can be applied to how THC affects the CB1 and CB2 receptors. Think of THC as the text message that signals you, acting as the CB1/CB2 receptor, to respond. After receiving the message, you then work to accomplish the task that was asked of you.
Ok, perhaps radio waves from cell phone towers are slightly different that chemical signaling between the cells of the body, but you get the point. Anyway, these CB1 receptors are found throughout your body, but happen to be concentrated in the brain while CB2 receptors tend to localize in the immune system. When THC locates and binds to these receptors, it triggers them to inhibit another protein called adenylyl cyclase. Adenylyl cyclase may be hard to pronounce, but it is central in activating and stopping many responses carried out by the body. You can think of adenylyl cyclase as a sort of “headquarters” that receives the signals from many receptors and coordinates the variety of chemical signals it receives and translates them into physical actions, or in the case of marijuana, the well-known list of physical and psychological changes in the body such as appetite, pain and pleasure, memory, and mood.
But why are these receptors found in our body in the first place? Were they placed in us simply because God wanted us to experience the effects of cannabis? Of course not! The human body is very efficient, and the CB1 and CB2 receptors do in fact have a normal purpose that does not include marijuana. Normally, these receptors are stimulated by two chemicals called anandamide (AEA) and 2-arachidonoylglycerol (2-AG) that the body produces naturally. These two molecules are called endocannabinoids (endo = in, cannabinoid = cannabis-like, i.e.- cannabis-like chemicals produced in the body) are the intended targets of the CB1/CB2 receptors. Although these two molecules do not cause the same psychotropic effects found in THC, they still regulate many of the same body functions such as appetite, cardiovascular activity, sensation of pain, and even bone mass!
So then, how can we use this information for the advancement of modern medicine? Interestingly, researchers are looking into developing pharmaceuticals that are similar to THC, but that do not cause the psychotropic effects that complicate prescribing them to the general public. So far, a drug called cannabidiol is emerging as a likely contender for this job. Already we know that these drugs can stimulate appetite and can be used for the treatment of glaucoma or pain, but new findings suggest that they might also be useful in the treatment of cancer as well.
I don’t want to bore you to death with in depth explanations about each of these, but the moral of the story is that it is very likely that we will see advances in the treatment of many medical conditions by using the information gained from studying these cannabis-like molecules.
It all started with a little plant called cannabis. And when we just so happened to set it on fire, we discovered that there were some effects! It was this creativity that sparked a revolutionary movement to learn more about the human body, unearthing a new class of useful medications and functions in the process. Cannabis certainly is a controversial little plant in popular culture, but its usefulness will likely help us to achieve the next pinnacle in medicine, or perhaps appropriately put, a new high.
Final thoughts on Endocannabinoids written by Steven Dotzler
Marijuana the Miracle Drug?
It seems that every day a new state is legalizing marijuana, or a new study is coming out praising the medical benefits of marijuana. For those of you against the legalization of marijuana for medical purposes, I’m sad to say but it has been shown time and time again to be therapeutically useful. Now you may ask; how is that something we have been told for years is along the same lines as other recreational drugs that are supposed to ruin your life actually do something beneficial for you?
First things first let’s clear the air about the use of marijuana for medicinal purposes. The benefits of marijuana are due to the active chemical compound in marijuana known as THC (tetrahydrocannabinol). The reason THC can have therapeutic benefits is because it is in the class of chemicals known as cannabinoids and your body actually naturally produces its own cannabinoids for every day functioning of your cells, these are referred to as endocannabinoids. Endocannabinoids are naturally occurring cannabinoids found within (endo-) your body. The major functions of these endocannabinoids that are being targeted for the use of marijuana as a medical therapy are their ability to induce cell death and even protect cells from death. You are likely wondering; how on earth something can both protect cells from death but also induce cell death, this is because the receptors that endocannabinoids bind to are found all throughout your body on different types of cells and control a variety of cell functions. So, depending on the type of cell, as well as the type of receptor stimulated, cannabinoids can cause cell death as well as protect cells from death. This ability of cannabinoids to induce cell death is being looked at for a potential cancer treatment because some cancer cells, such as breast cancer cells, have been shown to react to the presence of extra cannabinoids though cell death. The ability of cannabinoids to protect cells is being looked at in medicine as a potential method of treatment for many neurodegenerative diseases such as Alzheimer’s and AL S because some of the causes of these diseases involve pathways that are activated by cannabinoid receptors of brain and nervous system cells, so if excess cannabinoids can protect these cells from being damaged, they could potentially be used to slow the progression of the disease or even prevent it.
Alright so this sounds great right? Marijuana kills cancer cells and protects cells being damaged by other diseases, it’s the perfect drug…..Not quite although cannabinoids have been shown to have some to these positive effects it, like any other drug, has its negative side effects. Along with its ability to cause death to cancer cells it also targets your immune cells and can cause death to them as well. As we all know as well marijuana has psychoactive effects on the brain such as paranoia and anxiety which are also negative side effects. So sadly, no marijuana is not a miracle drug and is not anywhere close to it, but some of its properties show signs of potentially useful medical treatments. There is a chemical compound that is supposed to have all of the benefits of cannabinoids without any of the “high” or other psychoactive side effects called cannabidiol. This drug is yet to be approved by the FDA or go through significant clinical trials but it has shown promise in early research. For more information on cannabidiol visit http://www.projectcbd.org/.
In the end a lot still has to be learned about cannabinoids and their benefits in medicine before they become a mainstream form of treatment.
ALS: Caring on Ice
Why should people care about ALS. It is a disease that affects a relatively small amount of the world population. People should care because it is a brutal disease. ALS hits hard and it kills. People should care about ALS like they should care about any other disease, empathy. We should care because it makes other people suffer.
The ice bucket challenge has done a great job of spreading the name of ALS. Everyone knows that the ice bucket challenge is raising awareness towards ALS. But that is about all that it does. I knew that the ice bucket challenge was about ALS but I had no idea what ALS was, who was effected by it, and what could be done to treat it. After taking this course, reading our article, and discussing ALS in class my understanding of the disease has grown immensely. Something needs to be done than just get the name ALS out there. What ALS is and what it does to people needs to get out into the world and become common knowledge.
An interesting yet sad truth about ALS is that we are not exactly sure what causes it. We know that ALS leads to motor neuron death and we know that there are many players that might cause this. This is where research into ALS can be very exciting and very daunting at the same time. There are many paths to choose from and who knows which one will lead to better treatment. One thing is for sure however the more we know about ALS the more likely we will be able to create a more effective treatment for this terrible disease.
ALS, More than a Social Media Phenomenon
By now, we have all either seen, been nominated, or actively participated in the ALS ice bucket challenge. We know that the money is going to a good cause, either to fund ALS research or help those who are affected by this awful disease. We know influential people who have had the disease such as Steven Hawking and Lou Gehrig. But how much do we know about the disease itself? Lets break it down into more bite sized pieces.
Description:
Amyotrophic Lateral Sclerosis (ALS) is a fatal neurodegenerative disease characterized by muscle weakness due to the breakdown and death of motor neurons (the cells that deliver signals from the brain to the muscles). This leads to loss of neuronal function and ultimately to paralysis. (Additional information can be found at the ALS website, www.alsa.org)
Cause:
The primary cause of necrosis (death) of the motor neurons is a phenomenon called excitotoxicity. Excitotoxicity in ALS, occurs when there is too much of a neurotransmitter called glutamate in the synapse (the junction between two nerve cells). This causes overstimulation of the cell, leading to problems with functional pathways further down the nerve cell. The primary receptor to glutamate that has been studied is called NMDAR. It is different than other receptors for glutamate because it requires co-agonists, or other substances in addition to glutamate, to trigger a response by NMDAR.

Current Treatment:
There is only one drug currently on the market that is used to treat ALS. The drug Riluzole acts by suppressing the release of glutamate and the receptors that respond to glutamate in the synapse. This method attempts to reduce the excitotoxicity that is caused by ALS in the synapse.
New Findings (co-agonists):
(Glycine/D-serine)
Both Glycine and D-serine are co-agonists which affect the NMDAR receptor. Glycine has been shown to promote the release of glutamate which can increase the risk of excitotoxicity in a neuron affected by ALS. On the other hand, high levels of D-serine have been linked with NMDA toxicity. This occurs because the over activation of NMDA causes a pathway that leads to cell death (ERK1/2-/p38)
(Zinc)
Zinc performs several important functions within the cell. A vast majority of zinc found in the body is tightly bound to zinc dependent enzymes. Missense mutations within these zinc dependent enzymes have been linked to 20-25% of ALS cases. It has been found that those zinc deficient enzymes can then lead to ALS.
(Polyamines)
Polyamines, such as spermine and spermidine, have been found to be allosteric modulators of the NMDAR receptor (they bind to the receptor in a site different that the normal active site and by doing so, change the shape and function of the receptor). It has been found that these polyamines enhance the activity of NMDAR, thus causing a pathway which leads to cell death. Unlike many other neurotransmitters, polyamines are found throughout the body and not just in the neurons. In patients with ALS, polyamines have been found in higher concentrations within red blood cells.

It is clear that there is no one cause ALS, and the pathways that lead to its symptoms are very complex and for the most part are not fully understood. Although fund raisers such as the ALS ice bucket challenge might seem trivial, they take steps toward finding an ultimate cure for the disease, and offer the families of those who are affected, with much needed support.
ALS – We Need to Care
I’m sure that in the past few months your news feed has been flooded with the Ice Bucket Challenge. It probably even got to the point where you couldn’t stand seeing it anymore, maybe even resent the whole concept. Why do you care about ALS, it hasn’t affected anyone you know….yet.
You’re probably right. According to the ALS Association, only about 30,000 people have ALS right now – that’s 2 in every 100,000. We all feel the need to support those causes that affect us, or that are mainstream, like Parkinson’s disease, breast cancer, leukemia, and whatever else that comes across the TV or our radio, but why not ALS. ALS doesn’t have that famous spokesperson like Michael J. Fox or Muhammad Ali. It doesn’t have billions of dollars funneled into research, and honestly, how does a bucket of ice help the cause?
I can’t answer those questions, but imagine this. You are completely tied up and your mouth is taped shut. You are in your house and some stranger is taking all your things, one by one. You know what is happening, but there is nothing you can do about it. That is ALS. Sufferers become a prisoner in their own body, fully aware of what is happening, but without the means to do anything about it.
There are so many ways that ALS occurs. The onset is not necessarily genetic, only 5-10% of cases are due to inheritance. Instead, your body mutates on you, changing a gene that then causes the most intense traffic jam of transmitters inside your brain and spinal cord. Research is difficult because once that mutation occurs there are so many different ways that ALS affects you, that stopping just one doesn’t fix the problem. Imagine the worst traffic jam in the largest city. All the cars don’t come from in same direction; they converge into one central location. Opening up one of the pathways does not ease the flow for a different route; in fact it may hinder it. This is what ALS does inside the nervous system, except there is no way to clear the overload.
Pharmaceutical companies have the difficult task of trying to develop drugs to alleviate this problem, only for them there are other problems as well. Our brains are very protected in our body. The ability for drugs to enter our brain is very, very limited. While this is great for a healthy brain, it makes the task virtually impossible for those that are affected. So far there has been one drug that has been able to extend the life for those affected with ALS for a whopping 5 months. Yup, that’s right, less than half a year.
So the next time you see an ICE bucket challenge show up on your news feed, don’t get upset or frustrated. Think of the two in every 100,000 that are trapped inside their own body, fully aware, but unable to let you know. Become the voice for those that don’t have a voice for themselves, and help become part of a cure.
Behind the Bucket: A mechanism behind ALS appears to be too much of a good thing
Before the ALS awareness social media frenzy, the term “ice bucket challenge” meant nothing more to me than the 5+ month reality of living in Minnesota, also known as winter. The ceremonious dumping of ice became a phenomenon of Facebook friends and celebrities alike, but many jumped on the ice bucket bandwagon without much thought to the disease behind it other than a donation. While the challenge spread awareness about ALS, many don’t actually know what happens in the disease. Let’s break the ice and break down ALS, shall we?
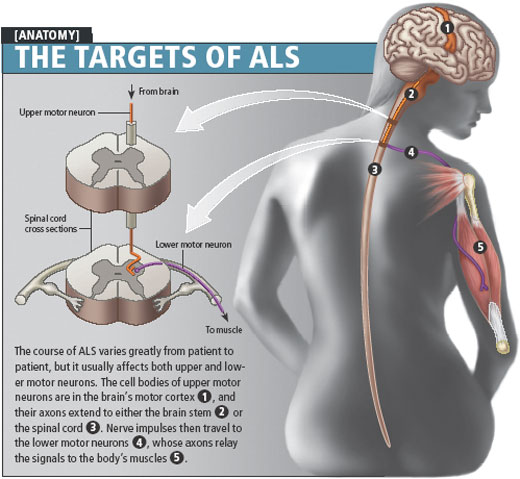
ALS stands for amyotrophic lateral sclerosis, an adult-onset neurodegenerative disease characterized by major motor neuron loss in the brain stem, spinal cord, and cerebral cortex. Motor neurons are nerve cells in the brain and spinal cord that send signals out to muscles, telling them when and how to move. As motor neurons degenerate and die in ALS, signals get sent at random, uncoordinated rates, and eventually no message is transmitted at all. When the signals are sent spastically, this causes muscle spasms, also referred to as fasciculations. When the motor neurons die, the muscles no longer receive signals telling them to move and they atrophy, or waste away. Defining characteristics of ALS are muscle weakness, spasms, and atrophy. The muscle atrophy gets progressively worse, and those affected have difficulties swallowing, chewing and speaking and eventually become paralyzed. The body withers away, but someone affected with ALS is painfully aware of losing motor functions and control, and within a few years, losing their life.

How are these messages sent and how does it go so wrong in ALS? Glutamate, a major excitatory neurotransmitter in the brain, is released and helps transmit a message from one motor neuron to another, eventually leading to muscle movement. It binds to two receptors, AMPA and NMDA. Glutamate is an important neurotransmitter that is also involved in many other important functions like learning and memory. When too much glutamate is present, it overexcites neurons and they die, a concept known as excitotoxicity. The article discussed in my Neurochemistry class at Concordia College focused on the role of NMDA receptors.
For many of you, the term “NMDA receptor” may provoke a similar reaction to that of the knights in Monty Python when confronted with the flesh-eating rabbit. Don’t fret; let’s use this castle theme to help explain the role of the NMDA receptor.


Think of a motor neuron as a castle and the NMDA receptor as the gate entrance. Glutamate is like a gatekeeper at the NMDA entrance; it is bound to the door and allows a certain amount of people in. The people represent calcium. As more people enter the castle, they create energy that excites the atmosphere inside the castle, and the excitement spreads. However, if there are too many gatekeepers at the entrance (too much glutamate), it becomes chaotic and they let too many people in the castle. The inside of the castle becomes overcrowded (too much calcium in the cell) and the energy turns from excitement to chaos, causing things to break in the castle. Eventually, the castle (motor neuron) is destroyed. In terms of ALS, massive amounts of motor neurons die in the spinal cord, causing motor deficits and eventually paralysis and death.
Unfortunately, the mechanisms behind motor neuron degeneration in ALS are not as simple as a castle analogy. NMDA is not the only receptor involved, and there are many other contributing factors to the progressive motor neuron loss. However, with more knowledge about receptors like NMDA and their role in the motor neuron death, we can more accurately target the mechanisms for treatment. Current treatments for ALS are limited but target the excessive amounts of glutamate (the gatekeepers in the castle example) in hopes of lowering glutamate levels and slowing the motor neuron degeneration. Though the general public cannot directly find the cure, we can support the cause by becoming educated on diseases like ALS in addition to supporting research funding.
Credits: The article discussed can be found here: http://www.sciencedirect.com/science/article/pii/S0925443912002736
Images used via Google search: ALS image from http://www.bestonlinemd.com/what-is-amyotrophic-lateral-sclerosis-or-als/
Monty Python image from: http://i.imgur.com/hJDbC6o.jpg?3
NMDA receptor image from: http://knowingneurons.com/2013/01/30/ltp-when-neurons-make-a-long-term-commitment/
**”Monty Python and the Holy Grail” is a British comedy and is not associated with ALS or its pathology**
{kind=link}
The True ALS Challenge
The ALS Ice Bucket Challenge has flooded social media outlets in the last few months and created a buzz around this neurodegenerative disease. It has jumped to the forefront of charitable causes, overshadowing many big organizations like the American Cancer Society.
But how much do people really know about ALS? I have watched dozens of videos of friends who have dowsed themselves in frigid water and pledged to donate to the ALS foundation to contribute to the cause. However, if anyone asked me what ‘ALS’ stood for or the effects of the disease two weeks ago, I wouldn’t be able to answer. I had no idea that about 15 people are diagnosed every day with Amyotrophic Lateral Sclerosis. I also learned that ALS, commonly known as Lou Gehrig’s Disease, mainly affects Caucasian males between the ages of 40 and 70.[1] Also, the majority of cases occur because of sporadic gene mutations. The next diagnosis could easily be a parent, a professor, a coworker, or a neighbor.
This great act of charity has raised a lot of money quickly, but where is that money going? The true results of these awareness campaigns lie in research trials that eventually lead to potential drug treatments. ALS is a frightening disease that decreases muscle function until the lungs and heart stop functioning. All the while, the person maintains their cognitive abilities. Research focuses on finding ways to decrease the extent and rate of motor function loss associated with the disease.
The one drug treatment available for ALS, Riluzole, is an antiglutamatergic drug. It acts by inhibiting the voltage-gated ion channel NMDA and reduces release of the neurotransmitter glutamate. As promising as this is, the exact mechanism of action is unknown. In the review article, the role of the glutamate acting on the NMDA receptor is discussed in detail. The grounds for this research are founded by evidence of high levels of glutamate in the plasma and cerebral spinal fluid of ALS patients as well as the toxic role NMDA plays in leading to cell death. The research focuses on glutamate’s excitatory actions in the spinal cord.
NMDA activation: https://www.youtube.com/watch?v=Q_z5ZL9STMw
Overexcitation of a cell by glutamate may lead to a number of pathways that lead to the same end result, cell death. One mechanism involves the endoplasmic reticulum (ER), the organelle responsible for modifying proteins into their functional form. Overactive NMDA receptors increase ER stress which depletes Ca2+ stores. Without proper balance of this ions ER cannot function properly which leads to improper folding of important proteins. This may have a connection to a common mutation in ALS patients found on the SOD-1 protein where it is not folded into its functional form.
Cell death from increased Ca2+ levels is more likely to occur when it is transported by over-active NMDA receptors than other receptor types. A similar toxic effect to ER stress is found in the mitochondria which produces reactive oxidative species during the oxidative production of ATP. These, along with numerous other pathways, link glutamate to the physiological effects of ALS. Because the only drug for ALS targets the glutamate-NMDA interaction and the contribution of NMDA in cell destruction, there is no denying its implications for possible drug treatments for the disease.
The real task is not completing the ALS Ice Bucket Challenge within 24 hours. It’s planting the seed of interest to the general public and pursuing that with ample research. If we use the Ice Bucket Challenge as a platform for discussion on this topic, then a wider audience may be reached and informed about this disease. I have discussed one area that is currently being examined for therapeutic purposes for ALS. I would like people to step away from the camera, and begin to dig deeper into the topic. To question where research is headed for ALS treatment. Without the ALS Ice Bucket Challenge as an attention grabber, I may not have had the opportunity to learn as much as I did and to share the most recent research. Continue to stay informed on the direction of research and keep on the lookout for the positive outcome of the ALS campaign in the future.
Overexcitation of a cell by glutamate may lead to a number of pathways that lead to the same end result, cell death. One mechanism involves the endoplasmic reticulum (ER), the organelle responsible for modifying proteins into their functional form. Overactive NMDA receptors increase ER stress which depletes Ca2+ stores. Without proper balance of this ions ER cannot function properly which leads to improper folding of important proteins. This may have a connection to a common mutation in ALS patients found on the SOD-1 protein where it is not folded into its functional form.
Cell death from increased Ca2+ levels is more likely to occur when it is transported by over-active NMDA receptors than other receptor types. A similar toxic effect to ER stress is found in the mitochondria which produces reactive oxidative species during the oxidative production of ATP. These, along with numerous other pathways, link glutamate to the physiological effects of ALS. Because the only drug for ALS targets the glutamate-NMDA interaction and the contribution of NMDA in cell destruction, there is no denying its implications for possible drug treatments for the disease.
The real task is not completing the ALS Ice Bucket Challenge within 24 hours. It’s planting the seed of interest to the general public and pursuing that with ample research. If we use the Ice Bucket Challenge as a platform for discussion on this topic, then a wider audience may be reached and informed about this disease. I have discussed one area that is currently being examined for therapeutic purposes for ALS. I would like people to step away from the camera, and begin to dig deeper into the topic. To question where research is headed for ALS treatment. Without the ALS Ice Bucket Challenge as an attention grabber, I may not have had the opportunity to learn as much as I did and to share the most recent research. Continue to stay informed on the direction of research and keep on the lookout for the positive outcome of the ALS campaign in the future.
[1] http://www.alsa.org/about-als/who-gets-als.html
Link to article mentioned: http://www.sciencedirect.com/science/article/pii/S0925443912002736
Link to article mentioned: http://www.sciencedirect.com/science/article/pii/S0925443912002736
I Challenge You to Learn About ALS and the Ice Buket Challenge
The neurodegenerative disease, amyotrophic lateral sclerosis (ALS), has been the center of YouTube videos and Facebook feeds for the past few months. It has been brought to focus by the Ice Bucket Challenge, which was created by Pete Frates, a victim of ALS. The challenge includes pouring ice water on oneself after being challenged. If you do not complete this challenge within twenty-four hours, the person is supposed to donate money to the ALS Association. Before we get into a brief view of the science behind ALS, here are some of my favorite Ice Bucket Challenge Videos.
Shay Carl Ice Bucket Challenge
Benedict Cumberbatch Ice Bucket Challenge
Before the Ice Bucket Challenge, most people knew ALS as Lou Gehrig’s Disease. I knew it as that and didn’t know much about the disease until the challenge and reading an article about ALS. Those with ALS have massive loss of motor neurons in the central nervous system, which includes the brain steam, spinal cord, and cerebral cortex. Symptoms include muscle weakness, muscle wasting, and muscle spasticity. These usually result in issues with breathing, swallowing, and speaking. Eventually, a person will lose the ability to control their body. Most ALS patients die within three to five years after diagnosis. While the disease can be inherited, it is usually sporadic.

The article that my neurochemistry class read described research focusing on possible causes of ALS. I will highlight three possible causes that were mentioned. The first is glutamate toxicity. This means that glutamate, a neurotransmitter, is exciting the receptor too much. This result is neurons like motor neurons being destroyed. Another possible cause is a mutation of the SOD1 gene. This SOD1 gene allows for the SOD1 protein to be made. Think of SOD1 as a police officer who protects cells from dangerous toxins. When the SOD1 gene is mutated, the protein can’t do its job properly. It starts to collect in the cell and can cause cells to destroy themselves. The last possible cause of ALS that I”ll mention is NMDAR activation. NMDAR are receptors on the cell. For these receptors to work properly, there are certain molecules that change or modulate these receptors that need to be present. Scientists have found that these modulators have been changed in ALS. This means NMDARs can’t work properly and result in possible cell death.
The main point of this article was to show that there are many factors that could play a role in the development of ALS and there’s plenty of research that still needs to be done. This leads me back to the Ice Bucket Challenge. By August, the challenge has raised over 100 million dollars. While this is amazing and shows the power that people have when they come together, the ALS Association’s spending has come into question. Is all this money going towards research? Sadly, no. Last year, they donated 28% of their funds to research. While some of the funds do go towards administrative and overhead costs, they also fund ALS public education and patient care services. I want to highlight that it is possible to donate to research only, and information can be found at their website. I hope that you have abetter understanding of ALS and what the Ice Bucket Challenge is doing.
Sources:
NMDA and ALS article
http://en.wikipedia.org/wiki/Amyotrophic_lateral_sclerosis
http://www.alsa.org/
CTE to ALS, a Deadly Path
ALS, the current neurological disease du jour, has been thrust into the minds of Americans via the now-infamous “Ice Bucket Challenge”. While the cause of this disease is not yet known, researchers have discovered many different players that may be involved. Neurotransmitter receptors, specifically AMPA and NMDA receptors are now being looked at for their participation in ALS. It is being hypothesized that an over-activation of these two receptors can lead to unnatural and damaging pathways in the neurons involved in motor activity. This explains the motor function lost in individuals with the debilitating disease.
Another hard-hitting neurological disease that only lately is beginning to be really talked about may be related to, or even a precursor of ALS. This condition is known as chronic traumatic encephalopathy, or CTE. CTE is a result of repeated damage to the brain, usually concussions, and involves changes in cognitive and behavioral functioning. Some researchers now believe that individuals with CTE are at a much higher risk to develop other neurological impairments, such as ALS.
Research of ALS and CTE are both in their infancy relative to many other human diseases. The little we do know about ALS shows that there is not one cause, but many different aspects of normal neurological functioning that can go wrong. While CTE does not always lead to ALS, and ALS is not only a result of CTE, there is a connection between the two ailments. The ALS “Ice Bucket Challenge” has brought much needed attention to the area of neurological diseases and what environmental aspects might lead to them. Does this mean that we have to pull every boy and girl out of all contact sports? I don’t believe a drastic reaction is necessary until further results are out, but parents need to seriously consider their children’s sports and what safety precautions should be carried out to ensure their long-term brain development and health.
ALS: More Than Just the Ice Bucket Challenge
In the last few months, the Ice Bucket Challenge has swept the nation with everyone from celebrities to your neighbor – and likely yourself too – completing this “challenge.” While the Ice Bucket Challenge has done an amazing job creating awareness and donations for this debilitating disease, few people truly understand what is happening for patients with ALS. Or why raising funds for research is so important.
ALS is a fatal neurodegenerative disease that stands for Amyotrophic Lateral Sclerosis – more commonly called Lou Gehrig’s disease. It involves the death of motor neurons in a person’s brain and spinal cord, which in turn causes muscle weakness, problems with speaking and breathing, and even paralysis. Because only the voluntary muscles are affected (like the muscles in your legs and arms), patients do not typically have problems with their heart or digestive system. But the inability to move and be “trapped in one’s body” can be devastating. Breathing, although usually involuntary, we can consciously control, meaning that it is also affected by ALS. Eventually, the patient requires a ventilator to breathe.
According to the ALS Association, every year in the United States 5,600 people are diagnosed with ALS, and at this very moment 30,000 people in the country suffer from the disease. After diagnosis, patients typically live for two to five years. Although ALS can be familial, this happens only 10% of the time. For the other 90%, onset of the disease is completely sporadic.
Currently, there is no cure for ALS and only one drug approved for treatment – riluzole – but it only extends the patient’s life by a few months. Why is it so difficult to develop treatments for this disease? The actual “cause” of ALS is unknown. It is believed to be caused by an overabundance of glutamate, an important neurotransmitter in the brain. This excess glutamate causes a particular receptor, called an NMDA receptor, to become hyperactive. When this NMDA receptor is active more than it should be, it results in too much calcium flowing into the nerve cells which eventually contributes to the death of the motor neuron. Until relatively recently, scientists believed that a different receptor, the AMPA receptor, was the main receptor involved with ALS. The brain and the many pathways of different neurotransmitters are very complicated, which only makes determining what is causing ALS more difficult. Mutations in a certain gene, called SOD1, could also have an effect on the development of ALS.
Why is this important? Because there are so many different pathways and possible reasons for the development of ALS in a person, it is essential that we conduct more research to help to discover and determine the best way to treat ALS. Ultimately, a cure for ALS could be found, but only with continual raising of awareness and donations. When the Ice Bucket Challenge craze has died down – as it eventually will – it is important that we do not forget about ALS. It is not a disease that gets a great deal of attention, but that does not mean it isn’t serious. It is a disease that progresses quickly and one that we need to remain aware of. Remember why you completed the Ice Bucket Challenge – not just for likes on Facebook, but to ultimately help the many people who struggle to walk, talk, and breathe as a result of ALS.