Neurochemistry allowed me to integrate and apply the skills and competencies gained throughout the intersectionality of liberal education learning at Concordia in few ways:
Critical thinking
Liberal education emphasizes critical thinking and analysis. Neurochemistry required us to analyze complex information, synthesize information from multiple sources, and evaluate evidence. By applying critical thinking skills to this subject, we as students can strengthen our ability to analyze and evaluate complex issues in other areas.
Interdisciplinary learning
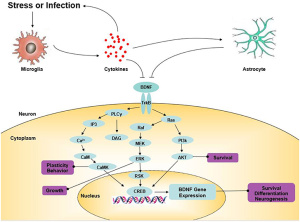
Neurochemistry draws on knowledge from various fields, including biology, chemistry, neuroscience, and psychology. As such, we can integrate and apply our learning from these different disciplines. This interdisciplinary approach is a hallmark of liberal education, and we can take these skills we gained throughout the semester learning and analyzing neurochemistry through different signaling pathways and social and environmental factors with us as we pursue other areas of study or work.
Effective communication
Liberal education places a strong emphasis on effective communication. Throughout the semester we needed to be able to communicate complex concepts and ideas to our classmates. By practicing effective communication skills in this context, we can enhance our ability to communicate effectively in other areas, such as in written assignments, presentations, or group discussions.
Ethical considerations
Neurochemistry has significant implications for society, including in the areas of healthcare, law, and public policy. A course in neurochemistry can allow us to explore ethical considerations related to these areas, including issues related to consent, confidentiality, and privacy. By considering these ethical questions, students can develop a deeper understanding of the importance of ethical decision-making in all areas of life.
In summary, neurochemistry allowed me to integrate and apply the skills and competencies gained throughout liberal education learning by providing opportunities for critical thinking, interdisciplinary learning, effective communication, and consideration of ethical implications that I will continue using in my future plans (wilderness therapy) and when interacting with human beings.
I was challenged and supported through this course that had a very refreshing structure. Neurochemistry was a discussion based class that involved cooperative learning, problem solving, and understanding different cultures and their approach to neurodegenerative disorders. It was so exciting to learn from students from different majors than just neuroscience. I gained insight from chemistry, biology, psychology, environmental studies, and dietetics. We all focus on our strengths and we were still willing to learn about different disciplines and work experiences.
My favorite part of this semester was experiencing how all four of my courses were intertwined. I was able to apply my knowledge and see the intersectionality from my Neurochemistry, Intercultural Communication, Religion, and Philosophy of Disability class. There was a lot of tension between these courses that gave me a deeper understanding of the problem of ableism, and the ways in which philosophical investigation could enhance the lives of individuals with disabilities and the fairness of institutions ranging from politics to the medical field. My liberal arts education is making me a more empathetic and aware being. I would love to see courses like philosophy of disability to be required courses for individuals that are planning on going to the medical field. These humanities courses would give insight and compassion to how diverse human experiences effect our systems and personal lives in this world structured for white, cis, able bodied individuals.