Image 1
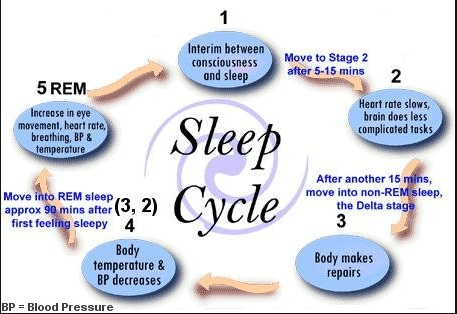
It’s finals week everyone, we made it to the end of the semester and are nearing the finish line. Because it’s finals week, and motivation is at an all time low I will be providing you relatable, and hopefully something you’ll find funny throughout the rest of this blog. I hope my efforts make your finals week just a little brighter. The question at hand is “how did this class allow you to integrate and apply the skills and competencies you gained throughout your education at Concordia.” Because as you have already realized after nearly completing this class, did more than simply learn what an action potential was and how ions flow in and out of the cell, huge win. 
Image 2
Let’s start with the Peak project shall we? If we’re being completely honest with ourselves almost none of us like group projects, unless we’re the one being pulled along throughout the entire process. But if we think about it for a minute, Concordia has put our group skills to the test from day one. We’ve had group projects throughout our entire collegiate career, some examples: working on a combined research paper, working on a danio rerio (zebrafish) project, working with those annoying little things in biology class with people who never came to class, etc.
Image 3
Whether we’d like to admit it or not, we’ve been doing group projects this entire time, theoretically this has prepared us for the real world. Because, like class, we will not always get along with our coworkers. We might have an annoying individual in our group, we might have to carry the entire workload and receive no extra credit or praise for doing so, it’s part of life and the real world that awaits us. As Forest Gump would say, “life is like a box of chocolates, you never know what you’re gonna get,” the same goes for coworkers in the real world. Our PEAK project allowed us to see the accumulation of our hard work throughout college, allowing us to see not only how far we’ve come in terms of improving our collaboration skills, but also how much we can still improve in the future after graduation. Not one group would say that the work was equally distributed, that they didn’t have at least one LAZY group member, or that everything went perfectly. And that’s alright, that’s real life and this class has helped us see and deal with that reality. The PEAK project encompasses the last three goals of Concordia’s liberal learning. I’ll paraphrase them but you theoretically all know what they are already; responsible participation in the world, understanding of interdisciplinary connections, and cultivating understanding. I will speak in terms of what my PEAK group accomplished because I don’t know what each of you did just yet.
Image 4; just remember, when you’re explaining the brain to someone who doesn’t know much about it, you can often overwhelm them
During our groups time working with Prairie St. Johns in Fargo, we were able to participate in the world, the real world, and not just some hypothetical setting in a classroom surrounded by sleeping students at 8 a.m. I will be perfectly blunt here, my group had MANY obstacles and challenges when it came to interdisciplinary perspectives and connections. The social work majors did not always see eye to eye with the neurochemistry students, and certainly the same can be said the other way around. But at the end of the day we figured out our differences and managed to deliver 160 meals to the local community, mental health de-stigmatization information, and information about local resources and shelters. We gave 140 of the 160 meals to the local homeless shelters, 5 shelters each received just under 30 meals each, some even got chicken wild rice soup hot out of the pot. And you know what the best part about the entire experience was? It wouldn’t have been possible without the help of all 8 members of the group. Sure not everyone carried their weight equally, but at the end of the day if those that did the bare minimum didn’t even do that much, those that did the most would have had to do even more. The entire experience gave all those who contributed a sense of self-understanding and some perspective in life. Let me explain, when we presented the shelters with the meals that we had prepared they showed us a level of gratefulness that was pure and heartfelt. It was as if we had just given them a new car or a new home, it was a moment that put everything into context and showed us as students that the problems that we face on a daily basis may not be as bad as we originally thought, essentially it gave us perspective. I realized that it is hard to compare my problems as a college student, eating 3 (or more) meals a day, to the hardships of those who live without proper housing. It was a humbling experience. 
Image 5; I mean, this one doesn’t need any explanation, come on
What other skills has this class allowed us to foster? Well for me at least this class allowed me to better understand research papers and scientific writing in general. We as a class probably take this for granted, but hand one of our readings to someone who doesn’t have a background in scientific writings and see just how confused they are by the MAPK pathway. I can promise you this, no matter how confused you are by that gobbly gook, they are 10x more confused. Unlike them you know that if you had to you could figure out every detail of that paper. Whether through additional research, breaking down the paper into individual categories like we do on Wednesdays, or extremely careful and slow reading of every detail in a piece of literature, at the end of the day you have the capacity to figure it out on your own. I unironically showed my dad what I was reading the other day and he damn near had a stroke, give yourself some credit you’ve come a long way. You probably see a piece of literature now and say to yourself, “I could figure that out, it might take me a week (or a semester) but I could do it.” These concepts relate directly to Concordia’s first two goals for liberal learning. Our love of learning has improved, whether you think you can or not you certainly have the capacity to read that paper on the MAPK pathway, and your intellectual capacity has grown significantly. I’m not just talking about this class, sure you picked some things up and honed your skills in new ways, but this class is the accumulation of your entire college experience, it is a way to see just how far you’ve come. 
Image 6; the only thing my neurons can seem to remember come test day
That’s it everyone, that’s my final blog post. One thing I’d like to comment on, I know that my posts can be a little goofy and light hearted, but that’s because I want to explain information effectively but also in a way that entertains the reader. I hope that you can all appreciate that I am trying to make this a good time, not only for me as the writer, but also for you as the reader. It is important that we as “scientists” explain complex information in a way that our audience can understand. I will need to be able to do this in my near future, if I as the doctor cannot explain to my patient what is wrong with them in an effective manner, I am doing my job incorrectly. Thank you all for a great semester, best of luck in your future and ROLL COBBS.




![Best Cannabis Leaf Pictures [HD] | Download Free Images on Unsplash](https://images.unsplash.com/photo-1597266029701-618ac066150a?ixlib=rb-1.2.1&ixid=MnwxMjA3fDB8MHxzZWFyY2h8MXx8Y2FubmFiaXMlMjBsZWFmfGVufDB8fDB8fA%3D%3D&w=1000&q=80)