
The Basics
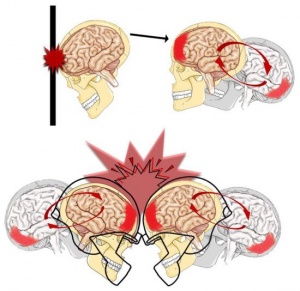
A concussion is a condition of neurological signs and symptoms that are caused by a biomechanical force to the brain. Symptoms of a concussion include headache, nausea or vomiting, dizziness, poor balance, light/noise sensitivity, fatigue, memory problems, confusion, etc. The cause of a concussion is a bump, blow, or jolt to the head or body that causes the head to move rapidly back and forth, as seen in Figure 1. The sudden movement of the head causes the brain to “bounce” around or twist in the skull causing injuries to the brain. The injuries to neural tissue caused by a concussion are predominantly functional or microstructural. Functional injuries include ionic shifts, metabolic changes, and impaired neurotransmission. Microstructural injuries include axonal stretch, axonal disconnection, inflammation, cell death, and cytoskeletal damage.
Concussions & Sports
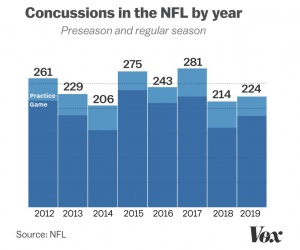
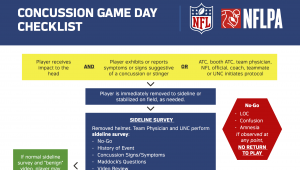
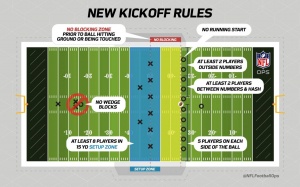
Between 1.7 to 3 million sport-related concussions happen each year with around 300,000 of those from American football. About 5 in 10 concussions gounreported or undetected. According to a study published in 2005, there are about 0.41 concussions per NFL game with 67.7% of concussions involving impact by another player’s helmet. 92% of players who sustain a concussion return to practice in less than 7 days. This data is shocking; however, it is from 16 years ago. The technology to prevent concussions in football and the concussion protocol have changed. Nevertheless, the deadly costs of repetitive hits to the brain are being revealed.
Chronic Traumatic Encephalopathy (CTE)
CTE develops gradually from an accumulation of blows to the head or repeated concussions. Symptoms vary between individuals but tend to resemble other degenerative brain conditions like Alzheimer’s disease: memory loss, depression, mood swings, personality change, fatigue, anxiety, frustration, etc. There is no diagnostic test for CTE, thus, a diagnosis cannot be confirmed until the post-mortem brain can be examined. Football players have a high risk of developing CTE as they are subjected to repetitive head injuries.
From a study of 202 brains from deceased players of American football, CTE was diagnosed in 177 players (87%), including 110 of 111 former NFL players (99%). The most common cause of death for participants with mild or severe CTE pathology was suicide, 27% vs. 47%. 86% of former NFL players hadsevere CTE, compared to 56% of former college players and 56% of semiprofessional players. The level of neurofibrillary tangles correlated positively with the severity of CTE. Neurofibrillary tangles (NFTs) are abnormal accumulations of the hyperphosphorylated (too activated) protein
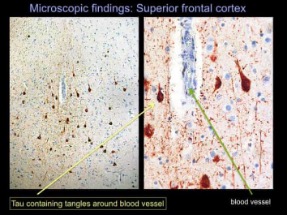
tau. Normally, tau supports the structure of the neuron by stabilizing microtubules which help guide nutrients and molecules down the cell. Within tangles, hyperphosphorylated tau detaches from the microtubules and stick to each other, forming tangles that block the neuron’s transport system from inside the cell. In figure 2 you can see the mass amounts of NFTs in a region of Aaron Hernandez’s brain. Additionally, there were deposits of amyloid- in all stages of CTE. This protein forms plagues that disrupt communication between neurons.
NFTs and amyloid- plaques are key markers of Alzheimer’s disease and associated with symptoms of impulsivity, depression, apathy, anxiety, explosivity, aggression, memory loss, and confusion. Among those that showed CTE pathology, 42.3% presented with cognitive symptoms in life, 43.2% showed behavior/mood symptoms, and 14.4% presented with both cognitive symptoms and behavior/mood symptoms.
Aaron Hernandez
A particular case study of CTE in a football player showed severe CTE pathology and the symptomology described with severe CTE. This case is of Aaron Hernandez.
Aaron Hernandez was a tight end for the New England Patriots until his career ended with his arrest for the murder of Odin Lloyd. Two years after his conviction for first degree murder, Hernandez committed suicide within his prison cell. Pre-mortem, professionals thought he had CTE, but this was confirmed after his death when
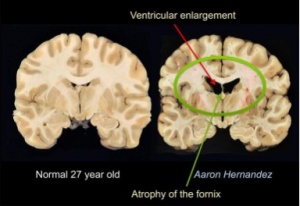
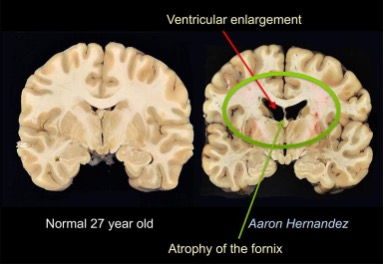
researchers were allowed to examine his brain. For a little bit of background Hernandez had been playing football since high school. He had many of the symptomology of CTE: changes in mood, aggression, depression, mood swings, personality changes, and memory loss. His brain: through Figure 3 you can see there is an atrophy of his brain specifically in the fornix and hippocampalregions. They also saw perforations of the septum pellucid and deposits of tau that you can see on this picture. Also, you can see that he had a lot of ventricular enlargements.
The researchers who examined Hernandez’s brain claim that it is the worst case of CTE they have ever seen in someone of his age of 27 years old.
After the death of Hernandez, his family filed a lawsuit against the New England Patriots and the NFL for being fully aware of the damage that could be inflicted from inflicted from repetitive impact injuries and not disclosing, treating, or protecting Hernandez from those dangers. They have since dropped this charge.
CTE makes a murderer?
I’m not sure that a neurodegenerative disease can make a murderer. In my opinion, neuronal dysfunction can be an aggravating trigger for homicidal tendencies. But this does not mean having CTE excuses such heinous acts. Instead, I believe CTE is a serious disease that is experienced by the many who experience repetitive traumatic brain injuries and shows itself as a change in key brain functions. CTE is something that should put fear in athletes, coaches, parents, and society. The development of CTE changes the brain and changes the person. And the truth is staring us in the face, if individuals continue to hit their head whether it be in combat, self-injury, accidents, or football they may see a change in themselves only explainable by CTE.
Sources:
https://www.nhs.uk/conditions/chronic-traumatic-encephalopathy/
https://heavy.com/sports/2020/01/aaron-hernandez-cte-photos-brain/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6916416/


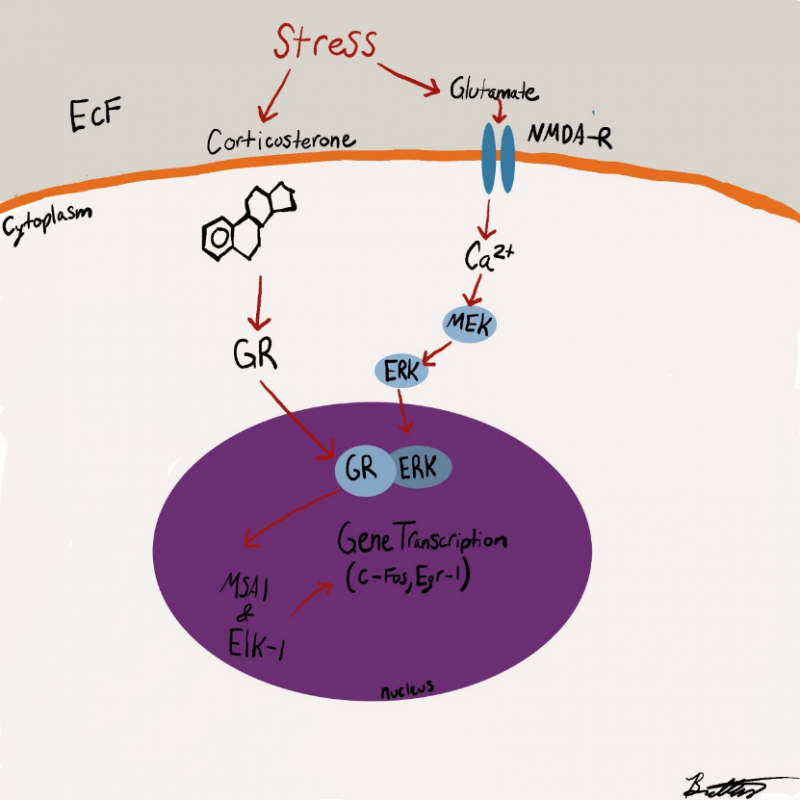
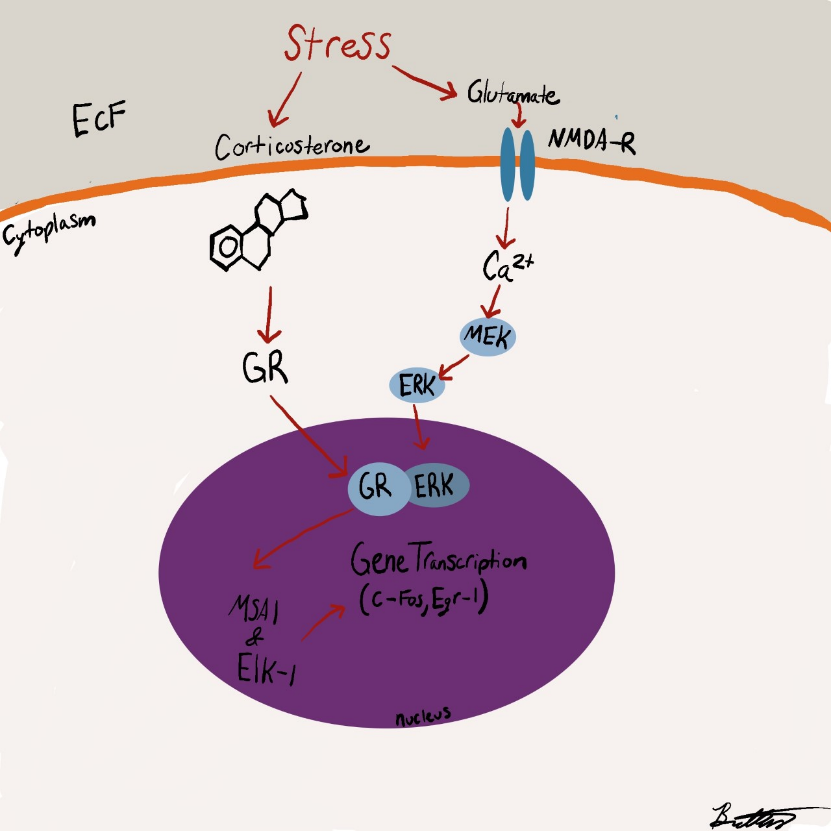



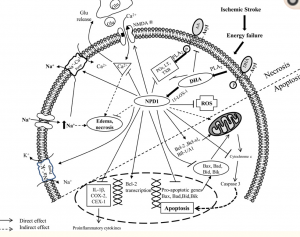





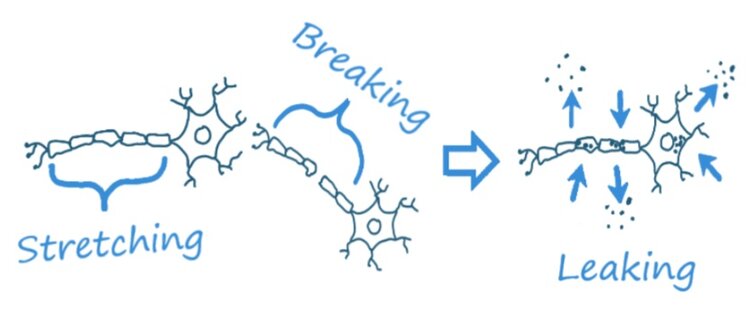 Ionic flux
Ionic flux 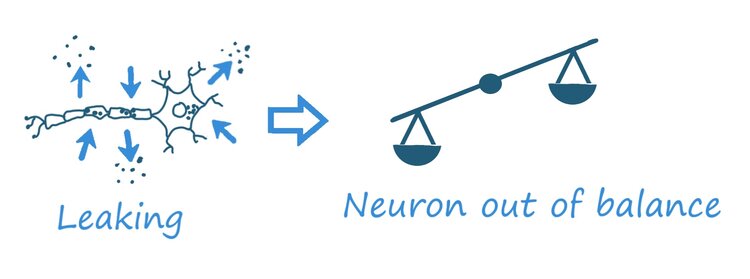 becomes “leaky”: notice imag
becomes “leaky”: notice imag