Cannabinoids in the brain
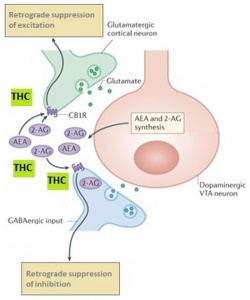
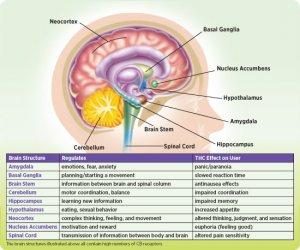
Cannabinoids are popular in both recreational and medical use. The primary active constituent of the hemp plant Cannabis sativa is delta9-tetrahydrocannabinol (delta9-THC). Psychoactive cannabinoids cause enhancement of sensory perception, difficulties in concentration, impairment of memory, along with an extensive list of other symptoms. Recent findings revealed delta9-THC-induced cell death with shrinkage of neurons and DNA fragmentation in the hippocampus (Ameri et al., 1999). The CB1 receptor mediates inhibition of adenylate cyclase, inhibition of N and P-type calcium channels, stimulation of potassium channels, and activation of mitogen-activated protein kinase. Interestingly, cannabinoids share a final common neuronal action with other major drugs of abuse such as morphine, ethanol and nicotine in producing facilitation of the mesolimbic dopamine system (Ameri et al., 1999). This might explain why people call it a ‘gateway drug.’
THC long-term effects studies

A study found that, cognitive impairments in adult rats exposed to THC during adolescence are associated with structural and functional changes in the hippocampus (NDA et al., 2021). They also found that when that animal is exposed to THC, there is an increased likelihood that the animal will target and self-administer other drugs that effect the same reward system. The studies referenced by the NDA found that some users developed altered connectivity within the brain leading to different cognitive impairments, while other studies found no significant structural differences in the brain. Basically, they have no idea if there is a negative long-term effect in general. However, they do believe that the age that you start using at is a determining factor.
Gateway drug?
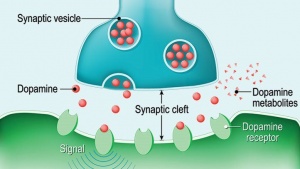
So, if no conclusive results were found on the structure of the brain long-term, what about long term effects on usage. They found that, early exposure to cannabinoids in adolescent rodents decreases the reactivity of brain dopamine reward centers later in adulthood. Although this does not directly conclude the results of a human brain, this could help explain the increased vulnerability for addiction to other substances of misuse later in life. These findings naturally would suggest that marijuana is a gateway drug, however, most people who use marijuana do not go on to use other, “harder” substances. They found that there is also a cross sensational effect within alcohol and other drugs. This means that simply drinking alcohol also heightens your responses to other drugs (NDA et al., 2021).
What to draw out of this
To say that marijuana has no negative effect on the brain would be disingenuous. However, just because the evidence is inconclusive at this point does not mean that it is entirely safe to use. If you use marijuana, cool, but just know there could be risks of future cognitive development in store.
Works Cited
Ameri, A. (1999). The effects of cannabinoids on the brain. Progress in Neurobiology, 58(4), 315–348. https://doi.org/10.1016/s0301-0082(98)00087-2
National Institute on Drug Abuse. (2021, April 13). What are marijuana’s long-term effects on the brain? National Institute on Drug Abuse. Retrieved from https://www.drugabuse.gov/publications/research-reports/marijuana/what-are-marijuanas-long-term-effects-brain.
National Institute on Drug Abuse. (2021, May 24). Is marijuana a gateway drug? National Institute on Drug Abuse. Retrieved from https://www.drugabuse.gov/publications/research-reports/marijuana/marijuana-gateway-drug.

 (2, 3, 4)
(2, 3, 4)