

If you ask an athlete if they know someone who has gotten a concussion, the answer is likely to be a resounding “yes.” Ask them if they know more than one person who has received a concussion, and the answer is probably “yes” as well. In fact, the athlete you are talking to might have even suffered a concussion themself at some point during their career.
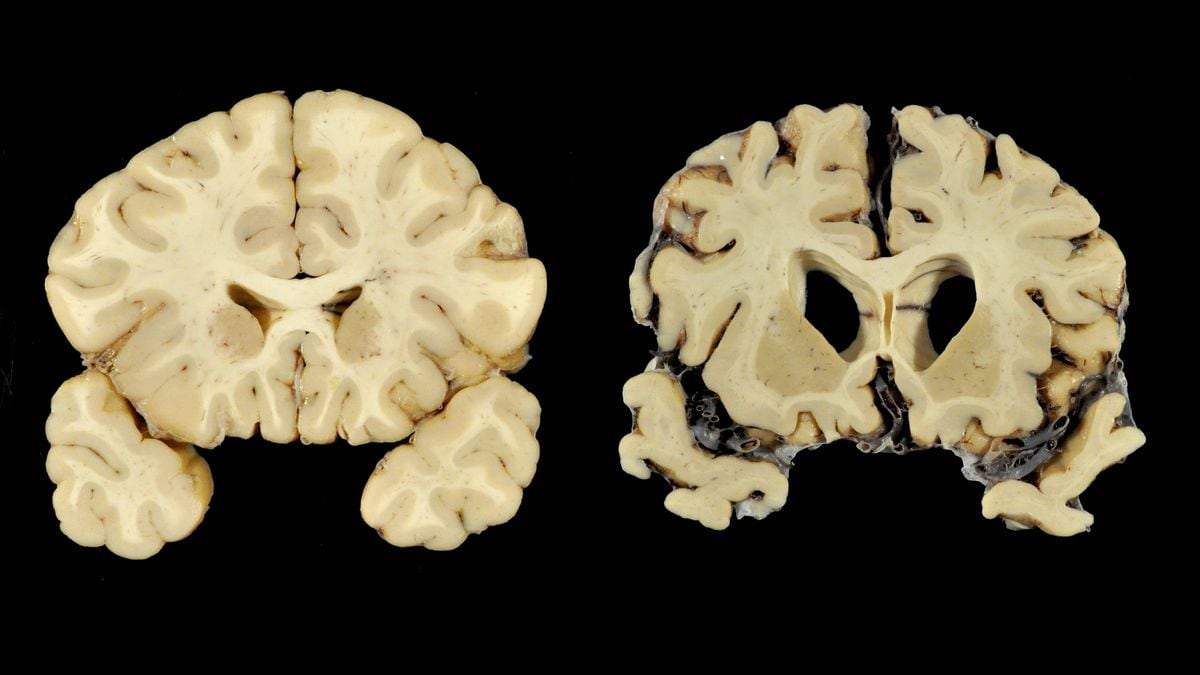
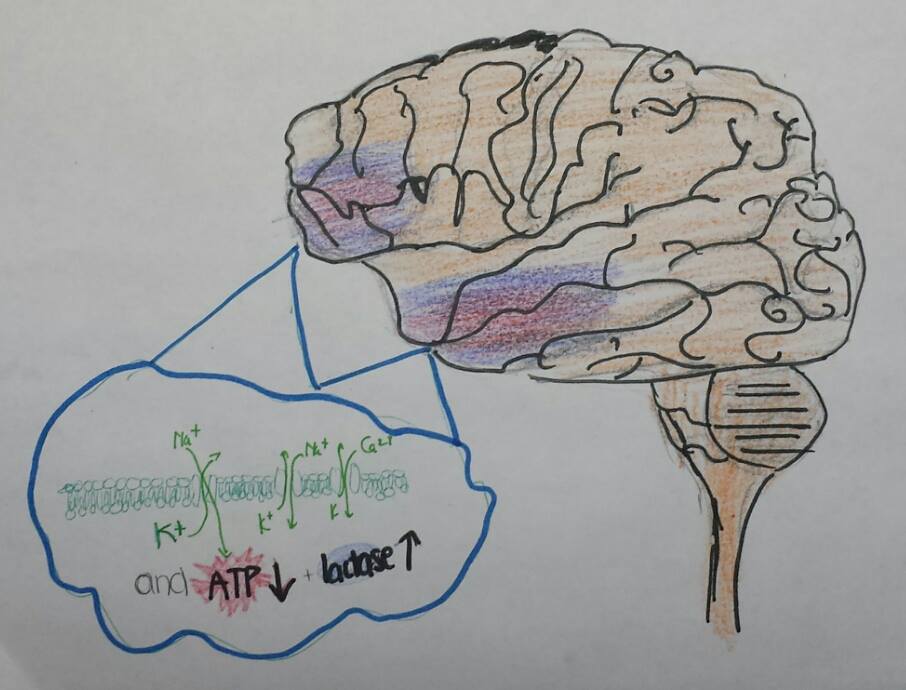
In 2011, it was estimated that 15% of all sports-related injuries were concussions (1). Another study found that on average, one player in every American football game receives a mild concussion (1). Although some athletes seem to recover from concussions relatively quickly, the damage that occurs to the brain can have a lasting impact on that person’s life, and even permanently affect their memory, cognitive abilities, and their personality (2). Concussions have a variety of physiological effects on the brain, including the damage and stretching of axons, upsets in ion balance and flux, higher rates of oxidative stress, higher energy demand and lower energy supply, and a lower oxygen supply to the brain (2). These physiological abnormalities can lead to permanent brain damage, especially in individuals who have suffered repeated brain injuries.

Given the prevalence of concussions among athletes, it’s important for anyone involved in sports to be aware of effective treatment options for concussions. This can give athletes a much better chance at achieving the best possible recovery from their injury. Here are some things you can do to minimize the impact of a concussion on your brain:
1. Eat foods rich in omega-3 fatty acids: Certain omega-3 fatty acids can help repair neuronal axons that were damaged by a concussion, and including them in your diet can even help prevent axon damage from occurring if you receive a concussion. Fish, and fish oil, are great sources of omega-3 fatty acids (2).

2. Rest: It’s extremely important to rest for an adequate period of time after receiving a concussion. This means avoiding sports or other physically strenuous activities that put you at risk for getting another concussion. It’s also a good idea to avoid tasks that require intense concentration, such as schoolwork or reading, as they can wear out your brain and slow the recovery process (3).
3. Wear a helmet while riding your bike: This one may seem obvious, but too many cyclists don’t always wear a helmet while riding their bike. This drastically increases their chances of receiving a concussion.
4. Return to activities slowly: Once you’ve recovered enough to start up your daily routine again, don’t immediately return to all of the activities you did before receiving the concussion, but rather start up your activities again slowly, one at a time.
5. Take pain-relievers: It’s usually safe to take nonprescription medications like aspiring or tylenol after receiving a concussion, and these drugs can help alleviate some of the painful symptoms of a concussion.
Concussions are difficult to deal with and can have a permanent impact on your brain, but with the right kinds of recovery strategies, you can often get back to your normal self in a relatively short amount of time!
Sources:
- http://prevacus.com/concussions-101/statistics/
2.https://moodle.cord.edu/pluginfile.php/625289/mod_resource/content/3/2014%20The_New_Neurometabolic_Cascade_of_Concussion.3.pdf
Image Credits:
- http://www.tvnewscheck.com/marketshare/wp-content/uploads/2017/10/CONCUSSION102010.jpg
- http://www.moveforwardpt.com/image.axd?id=3246dcf3-c76e-4eea-9324-f295f496e040&t=634757891481600000
- http://gettysburgian.com/wp-content/uploads/2016/03/fishoil.jpg
4. https://www.preeclampsia.org/images/M_images/aspirin_2945793b.jpg














{kind=link}
{kind=link}