
We all know that eating too much can cause obesity, stroke, heart failure, cancer and a load of other problems for our body, but does overeating have adverse consequences for our brain?
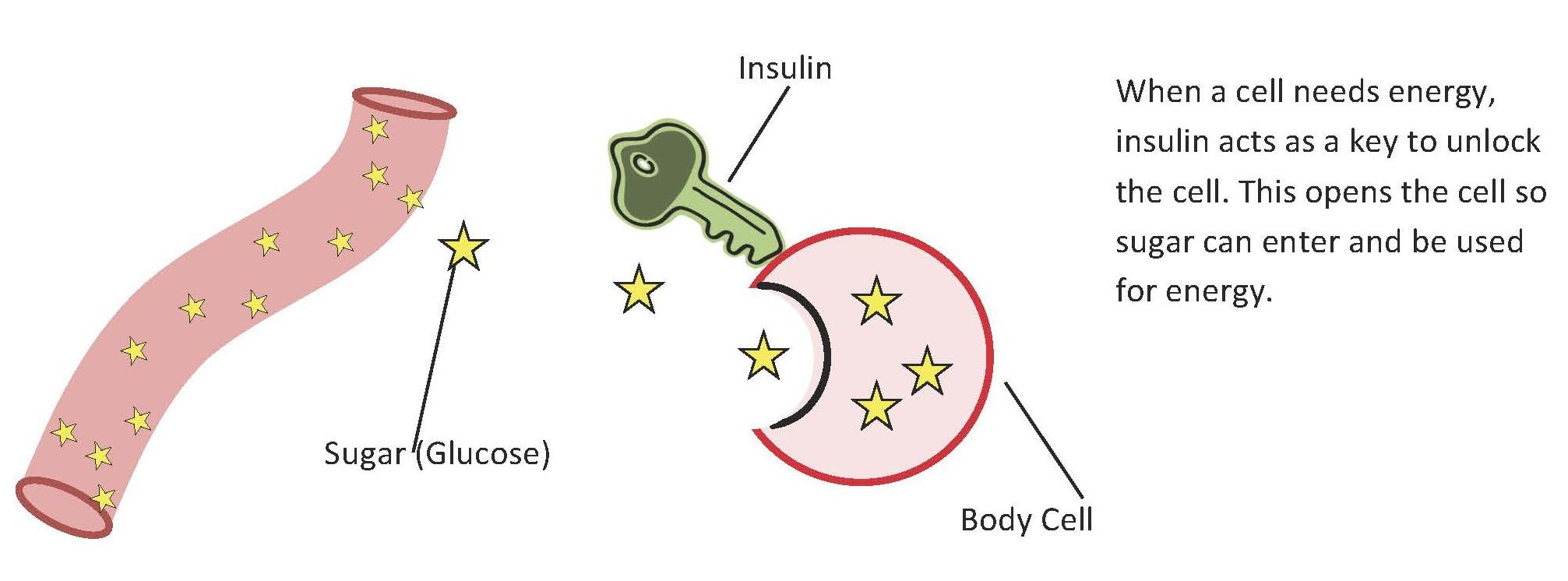
When we consume food it is broken down into smaller molecules, namely glucose, that can be used by individual cells for energy. When there are high levels of glucose in the body, a hormone called insulin is released. Insulin helps to break down glucose to a form that is actually usable by the body. It acts as a “key” for glucose to get to cells that need energy.

Like the rest of our body, the brain uses energy in the form of glucose to survive and function. Unfortunately, the “key” insulin, that is helpful in other places in the body, binds to cells that it is not supposed to when it is in the brain. Insulin turns on a cascade of signals called the PI3K/ AKT pathway. Recent research has shown that the PI3K/AKT pathway is expressed in high amounts in the brains of people with Alzheimer’s disease.
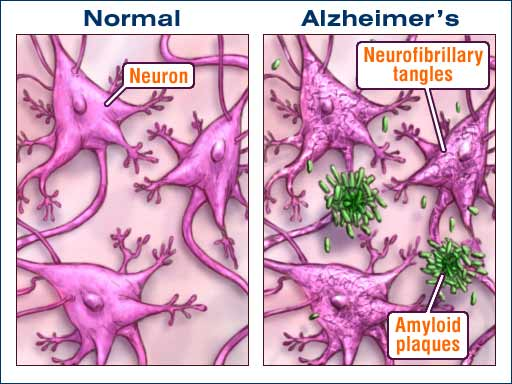
The PI3K/ AKT pathway, when active, can tell the brain cells to produce plaques and tangles in the brain. These plaques and tangles, made up of sticky proteins and malformed proteins, are hallmark signs of Alzheimer’s Disease. The plaques and tangles can lead to death of parts of the brain because they get in the way of the normal brain function.
Now, let’s go back to the overeating.
When you overeat, there is too much glucose in your brain, which leads to insulin release. Insulin promotes the PI3K/AKT pathway that can eventually lead to the accumulation of plaques and tangles and death of parts of the brain. People with Alzheimer’s disease have been shown to have a loss of brain matter and parts of their brain missing that are necessary for normal functioning. While working on only part of a brain, it’s no surprise that people with Alzheimer’s cannot form memories, are disoriented, or have problems with language.
So what? We need to skip Thanksgiving meal to save our brains? I don’t know that this is necessarily the solution to saving our brains. Instead, being conscientious of food choices and choosing healthy exercise patterns can help to regulate how insulin interacts with the PI3K/AKT pathway in our brain. If you start practicing these habits at a young age, your brain will thank you as it gets older. So go, overindulge on your turkey and stuffing, but when November 23rd is over, be sure to keep your health and brain health in check.
Information for this post was found here
For further information about plaques and tangles
For information on how to eat a balanced diet
Image link
Overeating as a Cause for Alzheimer’s Disease
















{kind=link}