Introduction to schizophrenia
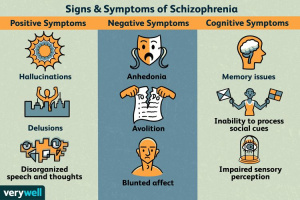
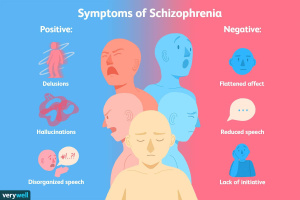
Schizophrenia is a psychiatric disorder affecting millions worldwide. Most commonly, schizophrenia is associated with positive symptoms such as hallucinations and delusions, and negative symptoms such as impaired day-to-day task functioning and decreased social interest. Although the disorder is common and easily identifiable and diagnosed, schizophrenia is not highly understood biologically, leaving effective treatments and preventative actions having yet to be discovered.
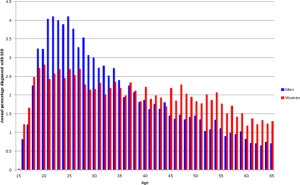
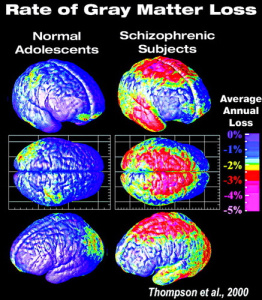
Schizophrenic patients are typically diagnosed in late teen or early adult years and symptoms can begin to arise years prior to diagnosis. But what causes or triggers the onset of this disorder in children or young adults? Studies have revealed that schizophrenia begins early in life with disrupted brain development (infection in utero, cognitive delays in early childhood, etc.). A key player in brain and cognitive development is the Wnt signaling pathway, and disruption of this signaling cascade is when schizophrenic symptoms develop.
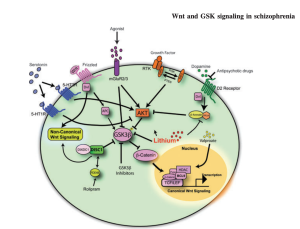
Wnt signaling and schizophrenia
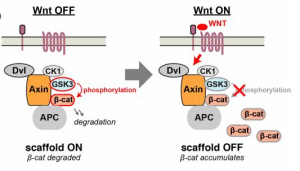
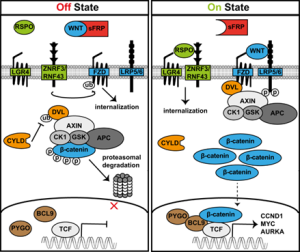
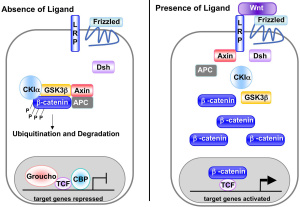
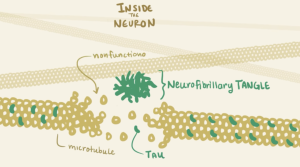
Wnt binds to frizzled receptors and recruits proteins to the membrane which causes dissociation of a beta-catenin destruction complex, and beta-catenin then transports to the nucleus for transcription. Without Wnt binding, this destruction complex containing the protein GSK3-beta, phosphorylates beta-catenin, targeting it for destruction. Beta-catenin gene transcription in the nucleus is crucial for cell proliferation, differentiation, and apoptosis (programmed cell death). Schizophrenia patients have been found to have decreased beta-catenin levels, implying Wnt signaling dysfunction in these patients.

Wnt signaling is essential for synaptic plasticity – change that occurs in response to neuronal activity at synapses that strengthen or weaken communication between neurons over time. With the dysfunction of Wnt signaling in schizophrenic patients, synaptic plasticity is decreased and with that decrease comes the loss of neuronal excitability. A doctor studying the correlation between Wnt signaling, synaptic plasticity, and schizophrenia symptoms inferred that the altered cognitive function, or the onset of negative symptoms, of those with schizophrenia begins with this loss of neuronal excitability. Then, the positive symptoms arise by the brain and body compensating for this loss of excitability – essentially, inhibiting the inhibition – which causes randomized firing that causes the hallucinations most often associated with schizophrenia.
References
Guildford, A. (2021, September 9). Schizophrenia: synaptic dysfunction plays a key role. Medical News Today. Retrieved February 19, 2023, from https://www.medicalnewstoday.com/articles/schizophrenia-synaptic-dysfunction-plays-key-role
Jia, L.; Pina-Crespo, J.; Li, Y. (2019). Restoring Wnt/B-catenin signaling is a promising therapeutic strategy for Alzheimer’s Disease. Molecular brain, 104(2019). https://doi.org/10.1186/s13041-019-0525-5
Singh, K. K. (2013). An emerging role for Wnt and GSK3 signaling pathways in Schizophrenia. Clinical Genetics, 83(6), 511–517. https://doi.org/10.1111/cge.12111

 Artstract by Timea Vrabcová
Artstract by Timea Vrabcová